Uncommon Manifestations of Intervertebral Disk Pathologic Conditions >>
Dorsal Epidural Disk Migration >>
>>
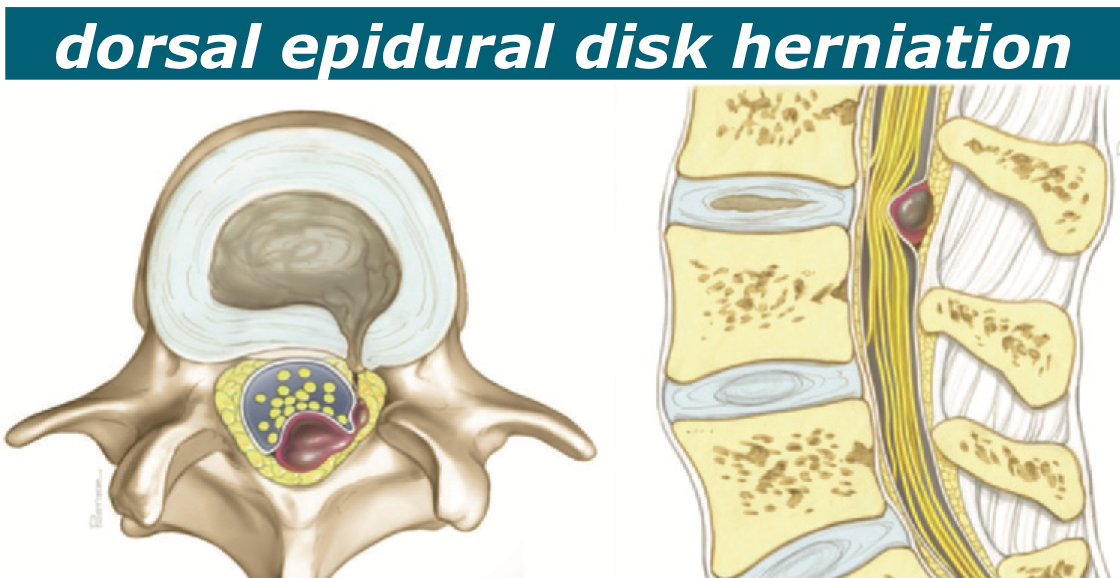
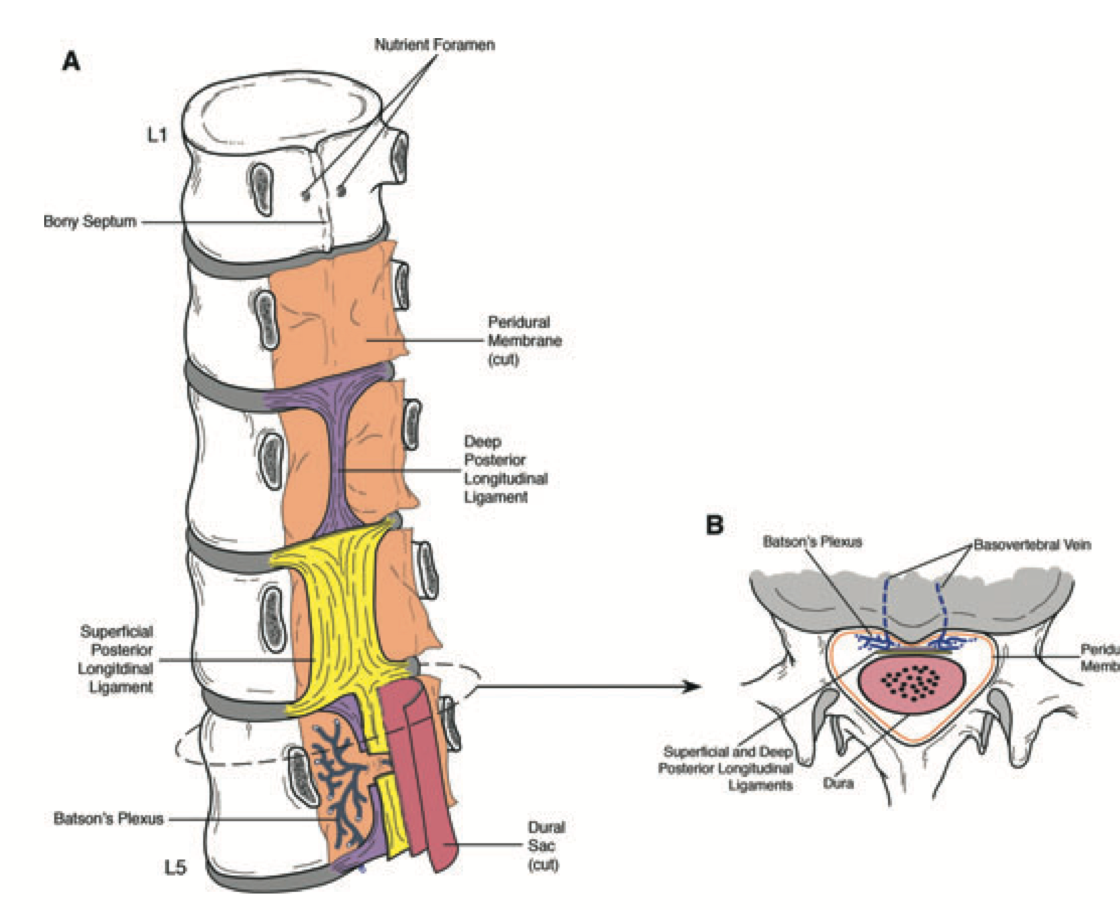
multiple barriers >> multiple barriers, including the posterior longitudinal ligament, the sagittal midline septum (septum posticum), the peridural or lateral mem- brane, the epidural fat and venous plexus, the dura, and the nerve root
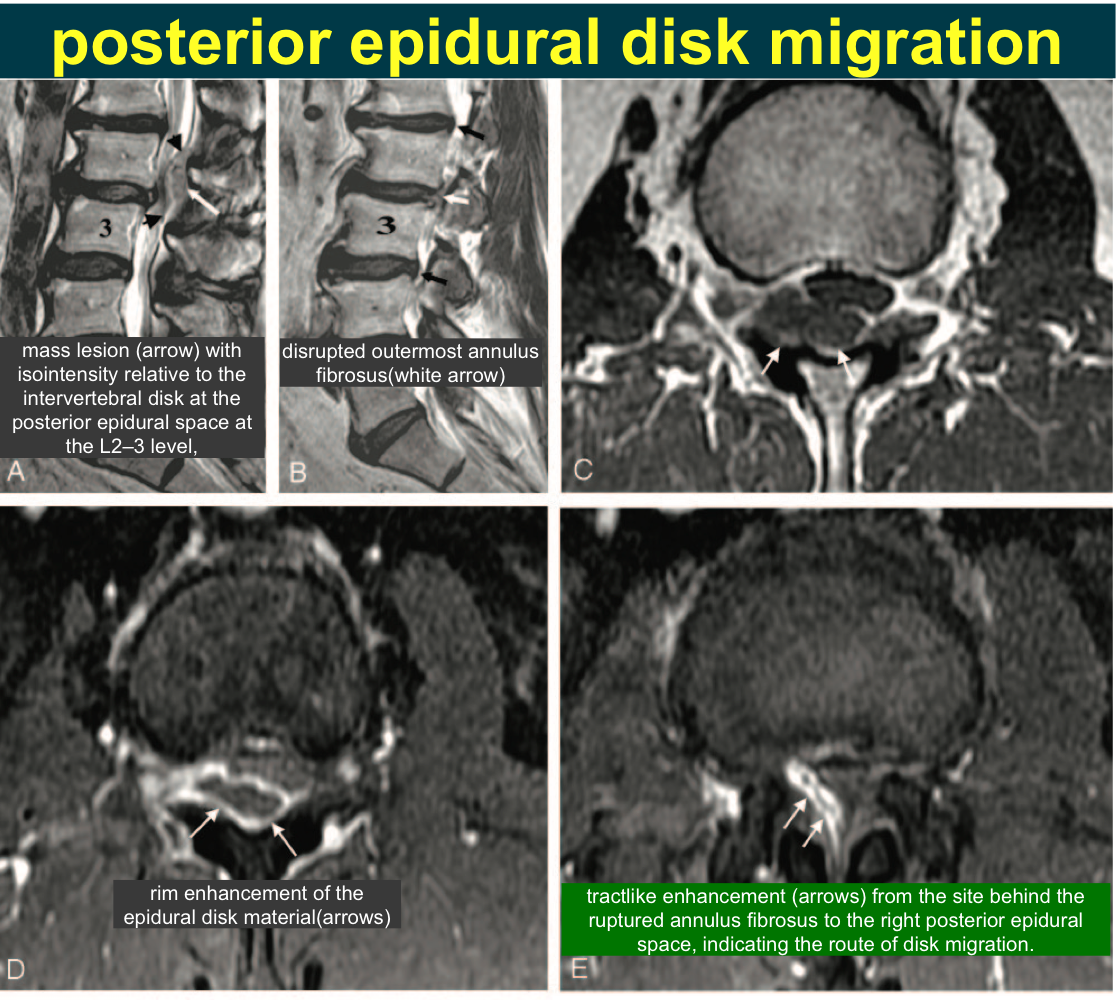
Imaging Features/Dorsal Epidural Disk Migration >> nonspecific mass in the dorsal epidural space
disk herniations often have an anterior and lateral soft-tissue component The signal inten- sity of the herniations is variable and nonspecific tractlike enhancement from the disrupted anu- lus fibrosus to the posterior epidural space if the mass contains gas, this finding can be a clue to diagnosis,
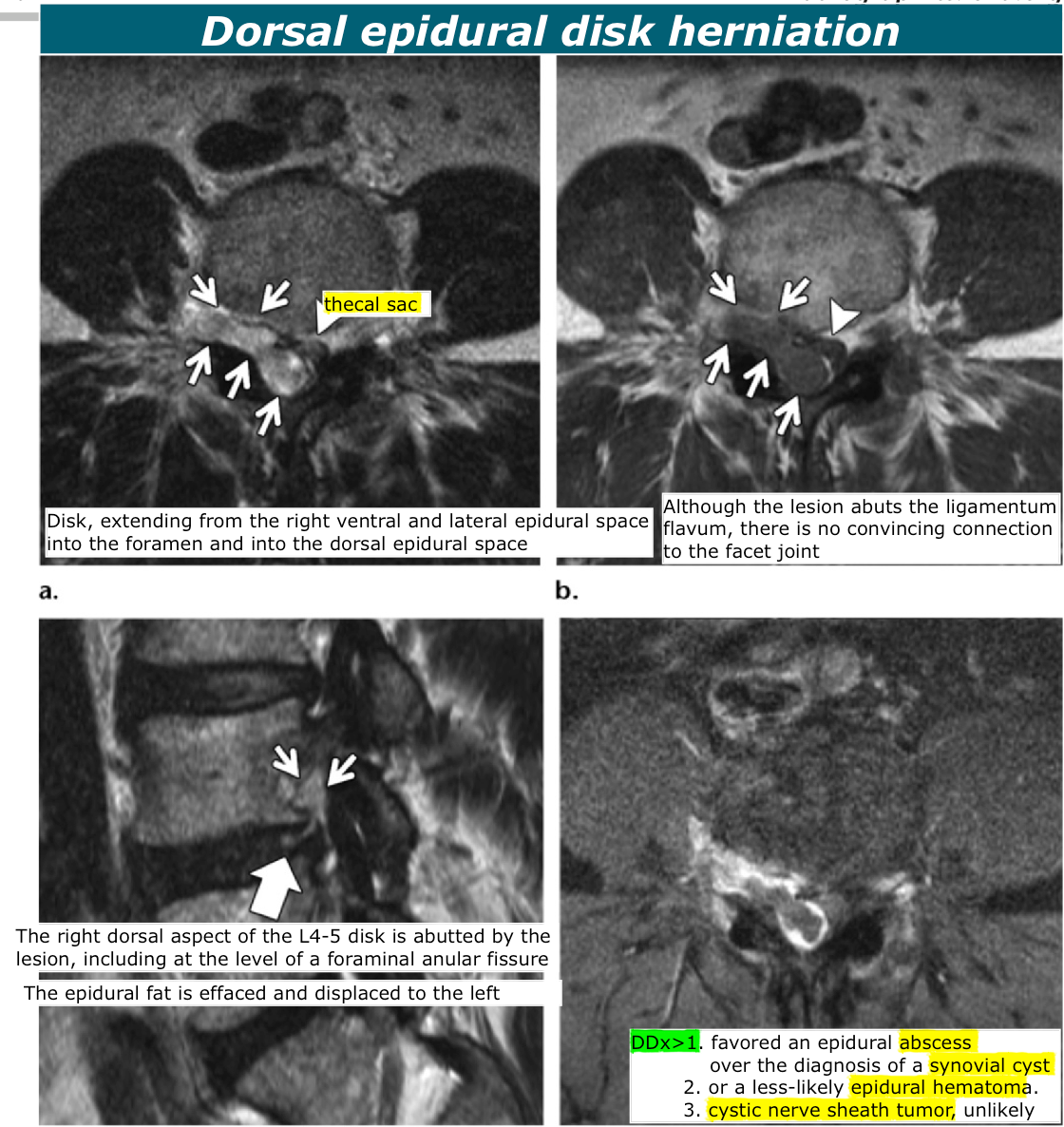
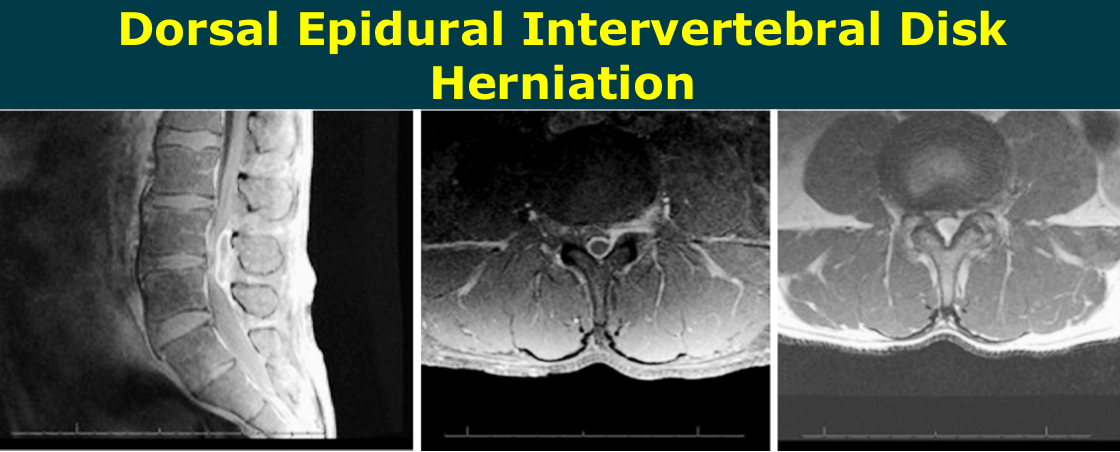
Dorsal Epidural Disk Migration >> Contiguous involvement of the ipsilateral ventral and lateral epidural space may be a helpful clue for the diagnosis of dorsal disk herniations
Synovial cysts may demonstrate a connection to an often arthropathic facet joint
Dorsal epidural disk herniation >>
posterior epidural disk migration >>
Dorsal Epidural Intervertebral Disk Herniation >>
Dorsally Migrated Epidural Disc Herniation with Intradural Extension >>
>>
>>
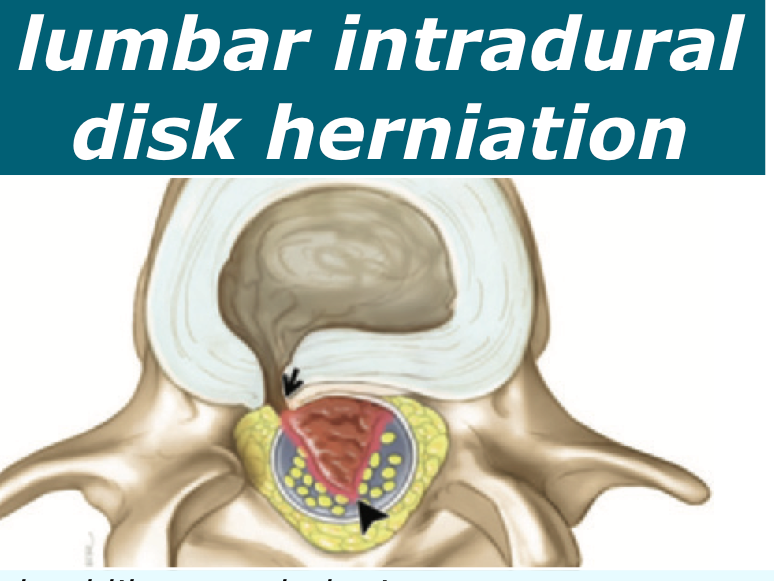
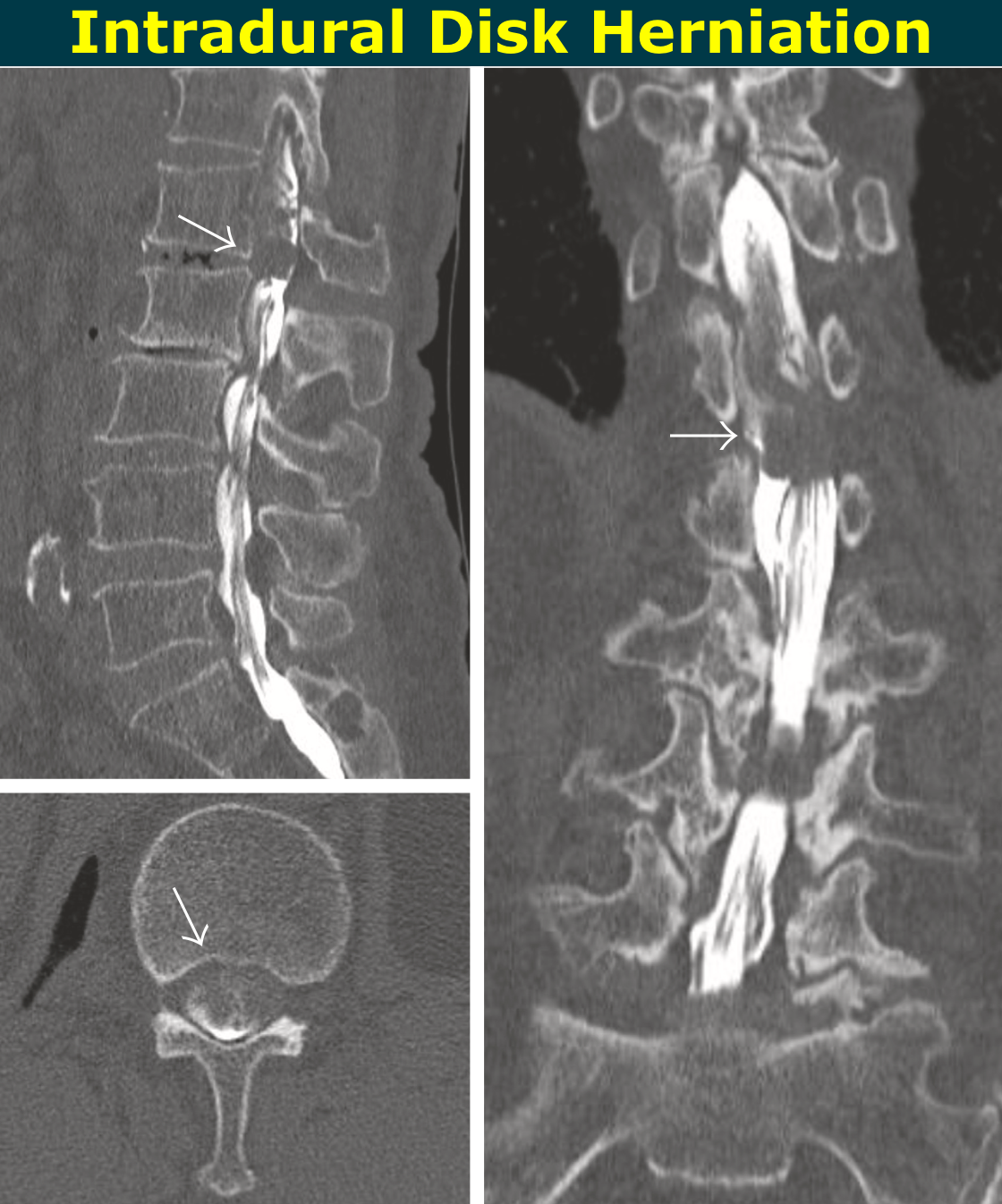
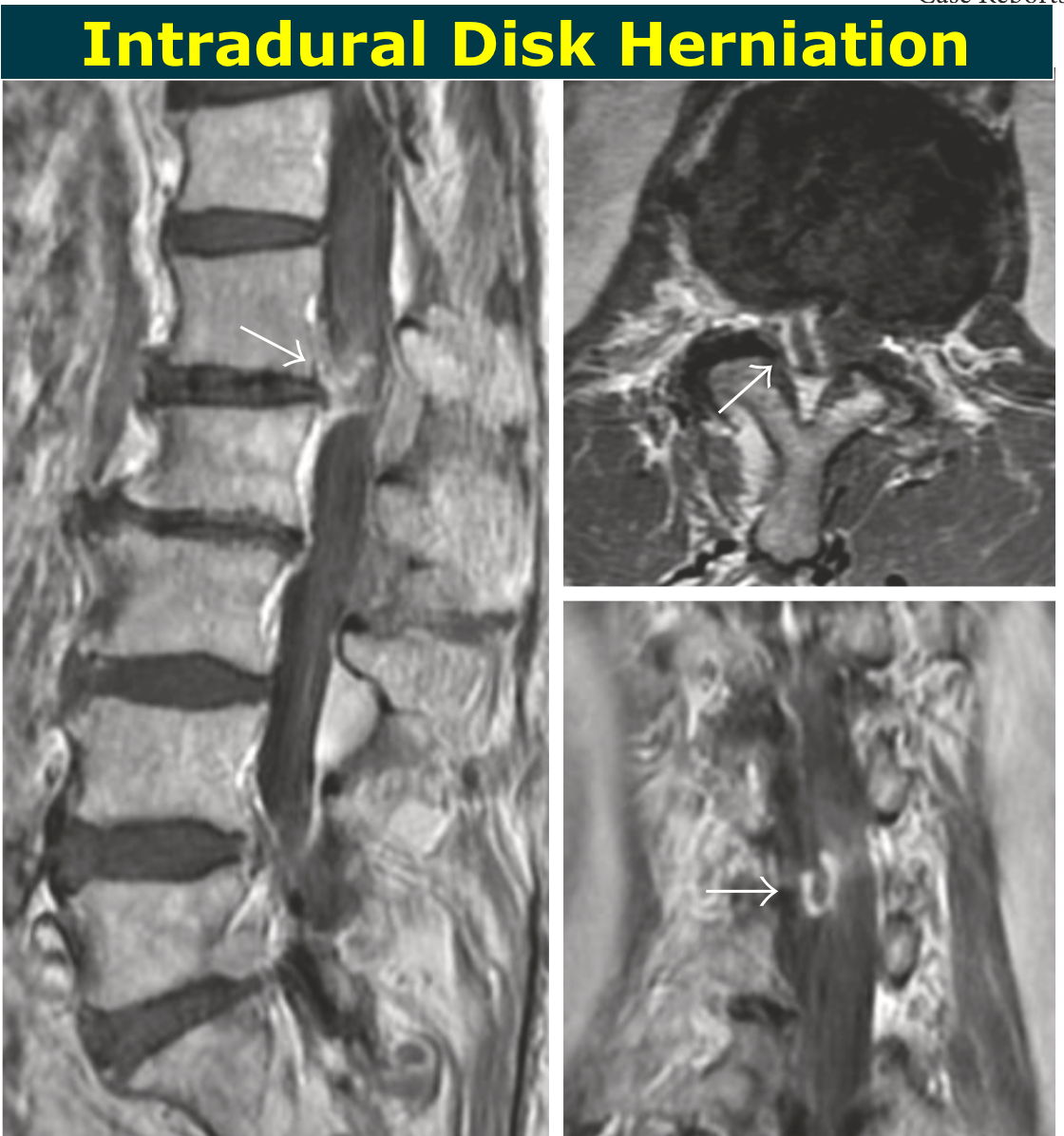
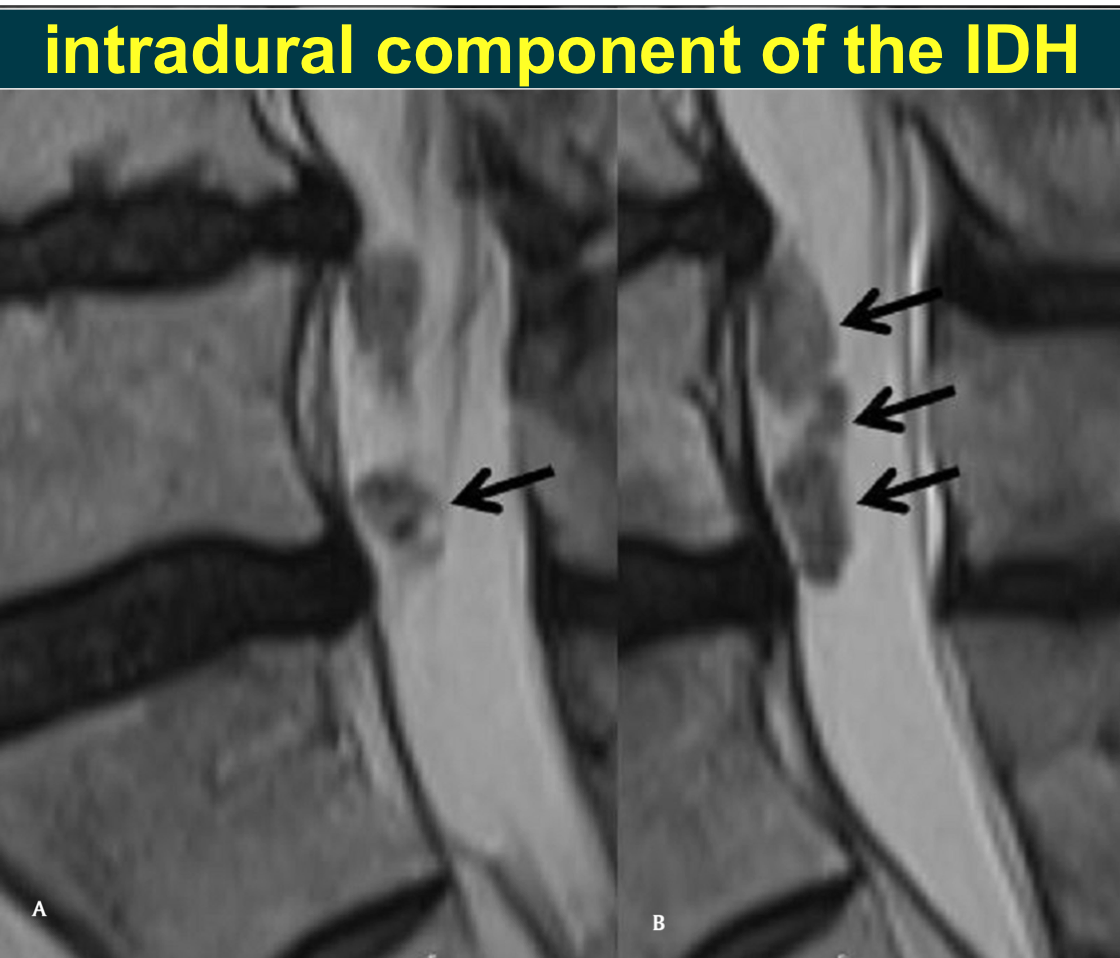
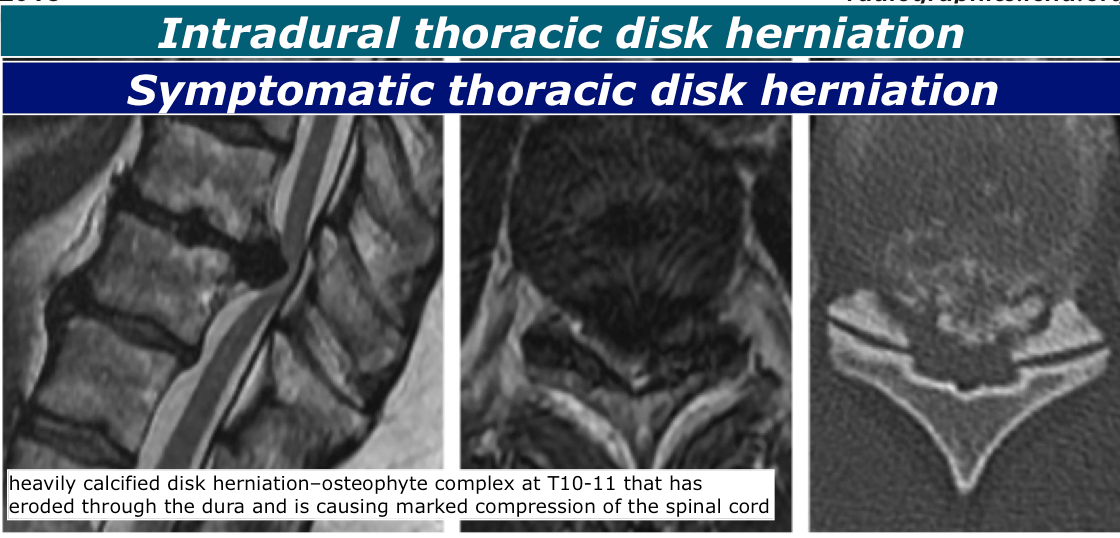
Intradural Disk Herniation >>
>>
Intradural Disk Herniation >> Causes of these adhesions could be inflammatory processes, developmental causes, a prior herniation, or trauma or surgery;
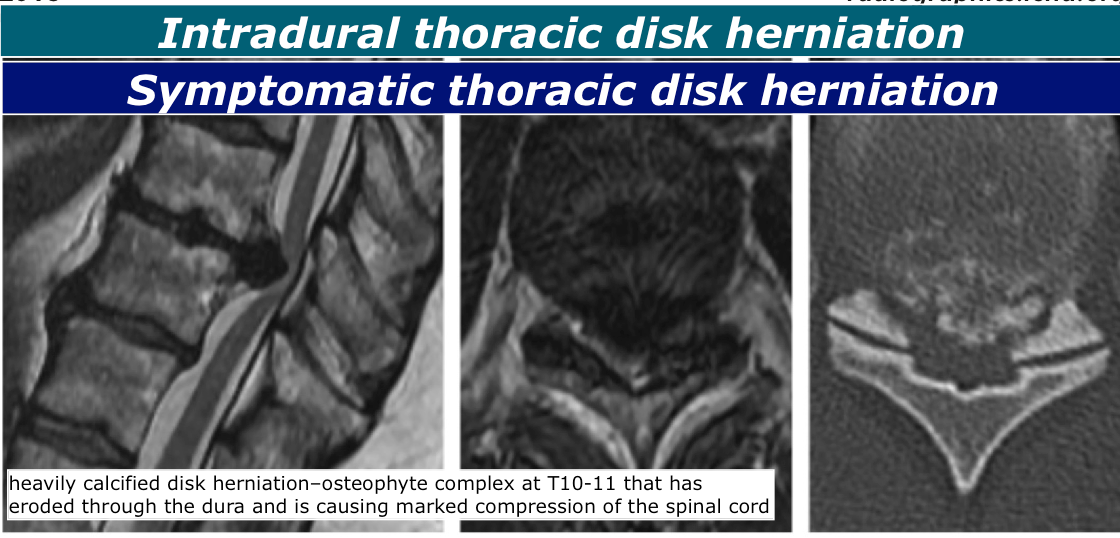
Most symptom- atic thoracic intradural disk herniations (discussed subsequently) are heavily calcified
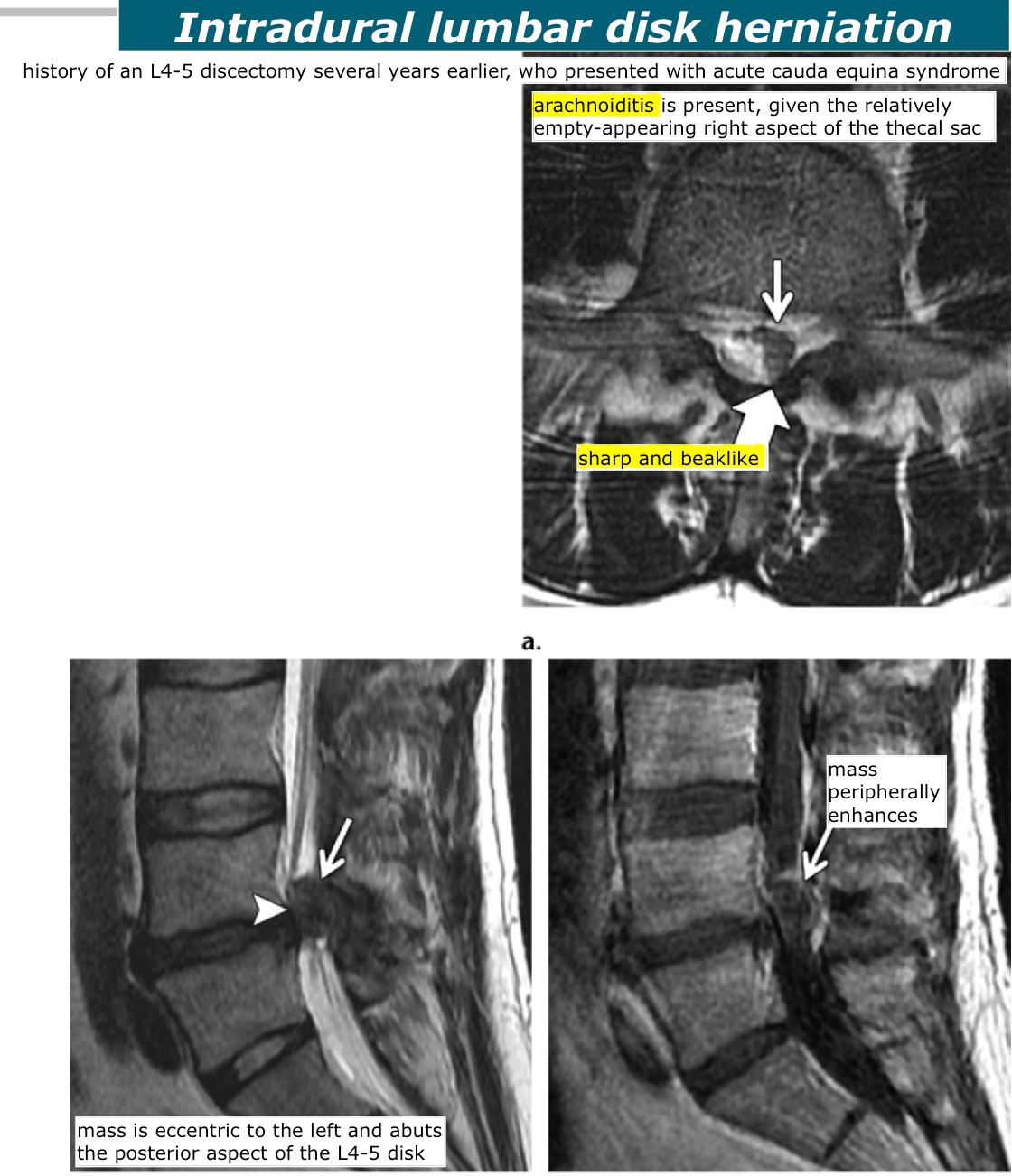
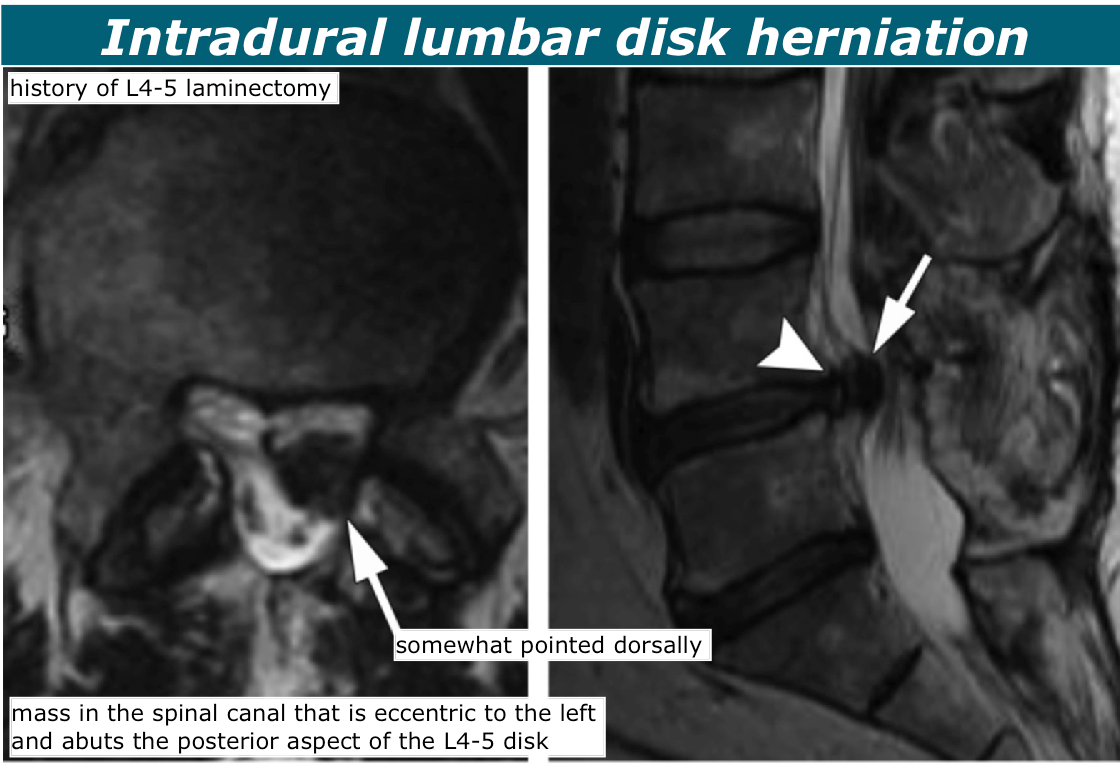
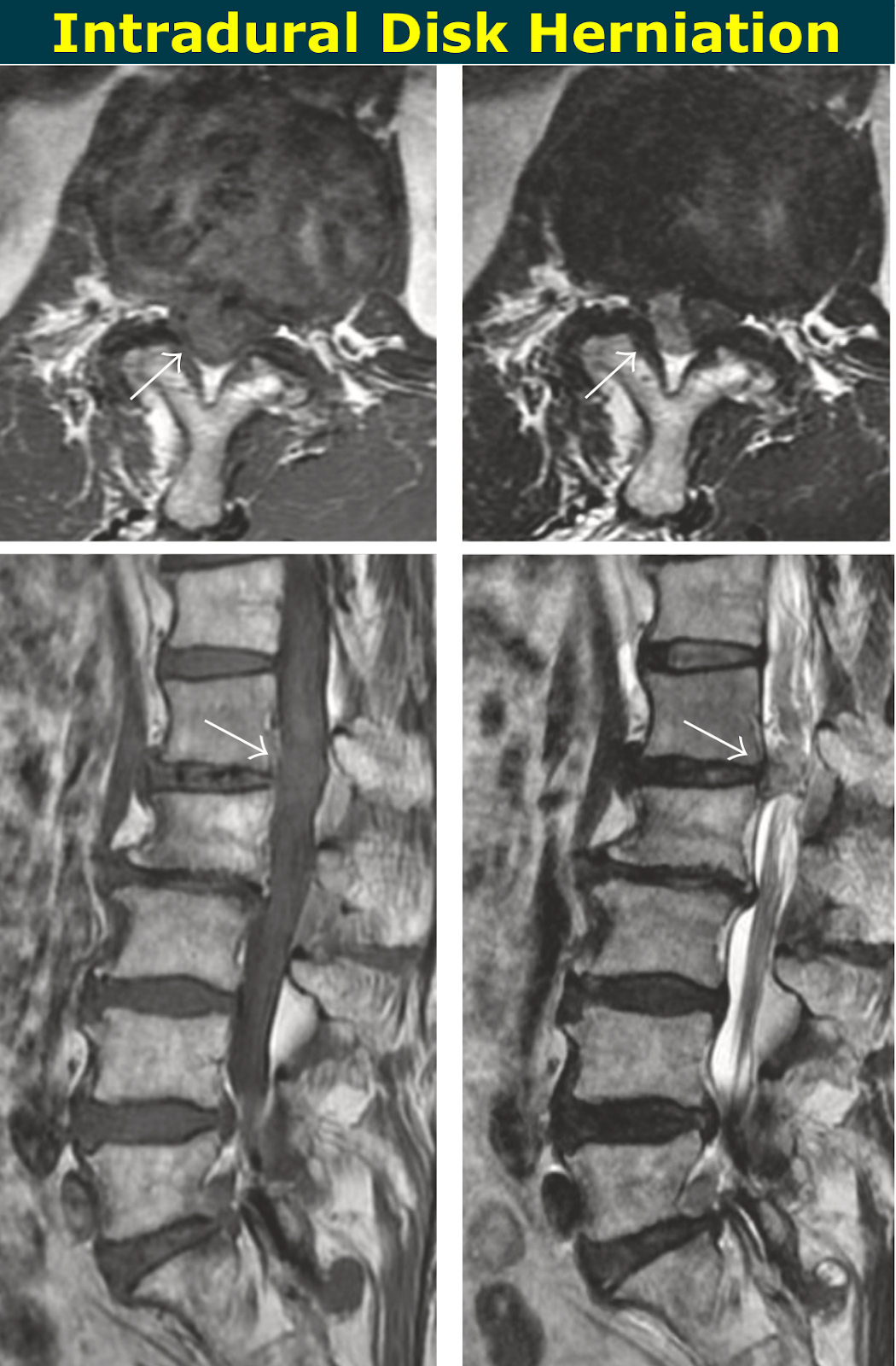
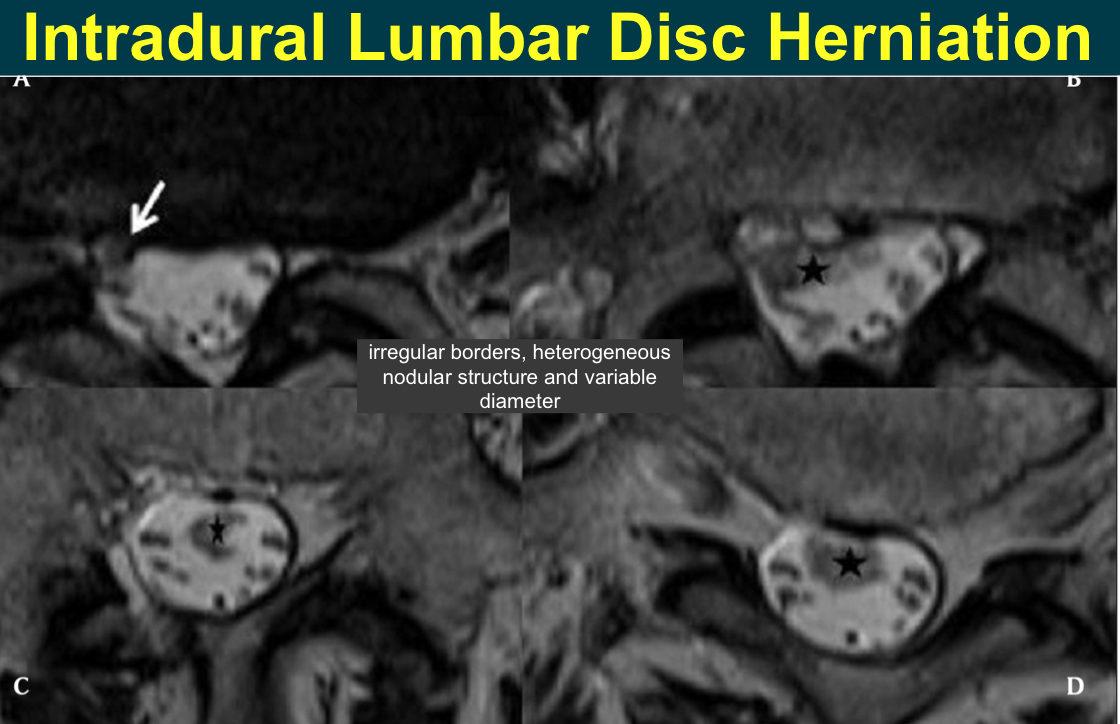
Intradural Disk Herniation >> intradural disk herniations are at lumbar levels (>90%), with L4-5 being the most common (~55%)
Thoracic disk herniations are most likely to be intradural (as many as 15%), particu- larly if the herniation is a “giant” herniation (as many as 70%)
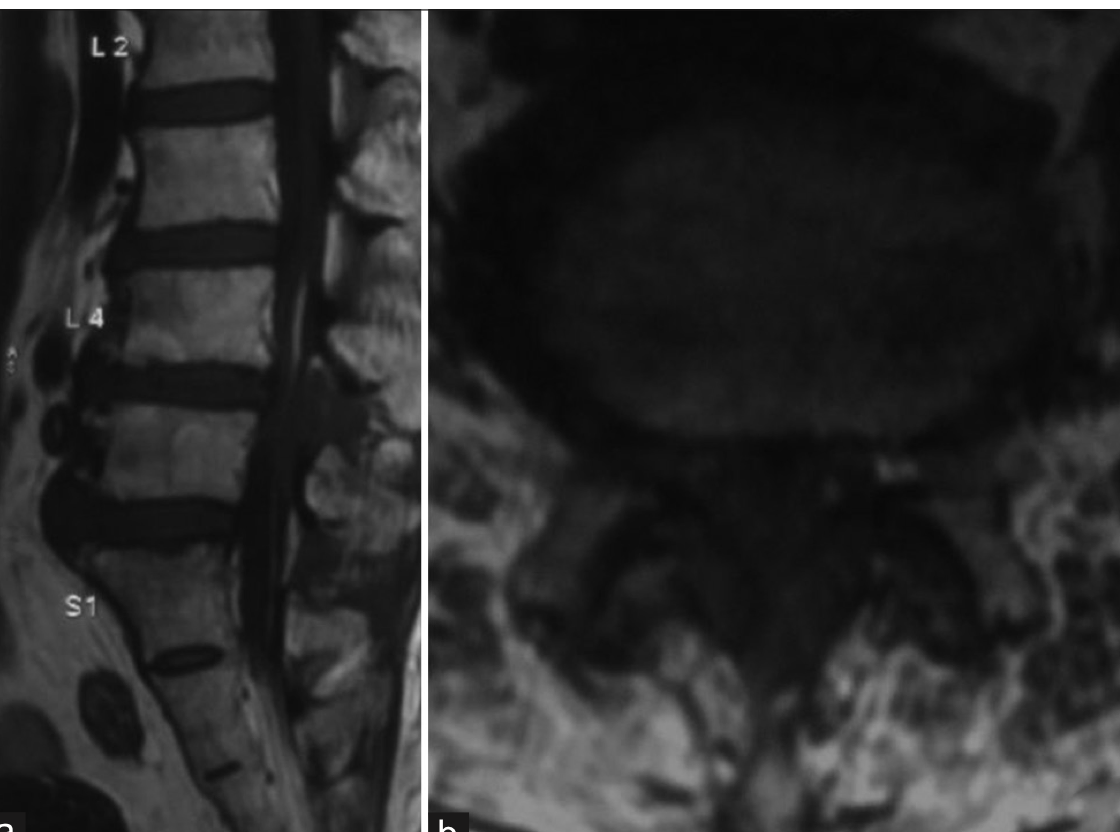
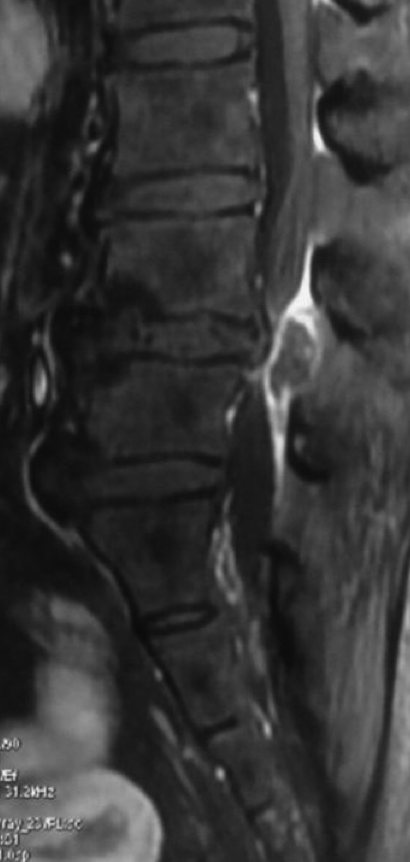
Imaging Features/Intradural Disk Herniation >> The typical clues of intradural location—widening of the subarachnoid space
A disconti- nuity of the posterior longitudinal ligament may or may not be depicted “hawk-beak” sign—a sharp beaklike mass at axial T2-weighted MR imaging—may be present
—> The authors who described this sign suggest that the sign may be due to a sharp car- tilaginous endplate component of the intradural disk herniation
Differential Diagnosis/Intradural Disk Herniation >> nerve sheath tumor, lipoma, inclusion cyst (epidermoid or dermoid), meningioma, arachnoid cyst, and metastasis
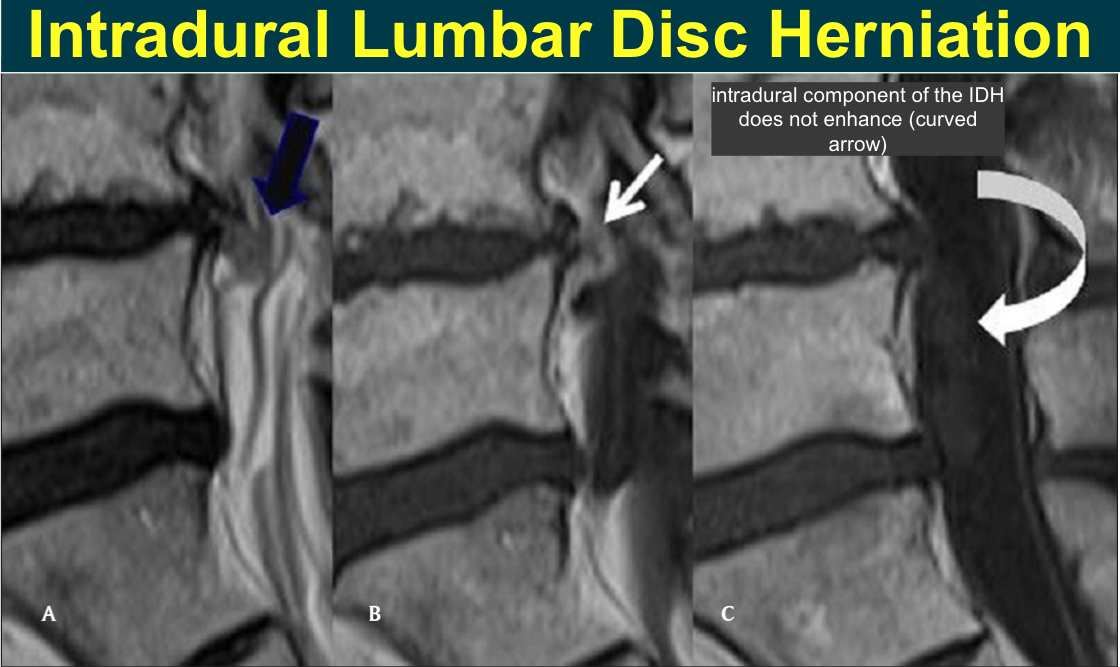
Ring enhancement is not typical in the most common of these entities, nerve sheath tumors and meningiomas
Intradural lumbar disk herniation >>
Intradural lumbar disk herniation >>
Intradural thoracic disk herniation >>
Intradural Disk Herniation >>
Intradural Lumbar Disc Herniation, >>
Discal Cyst >>
>>
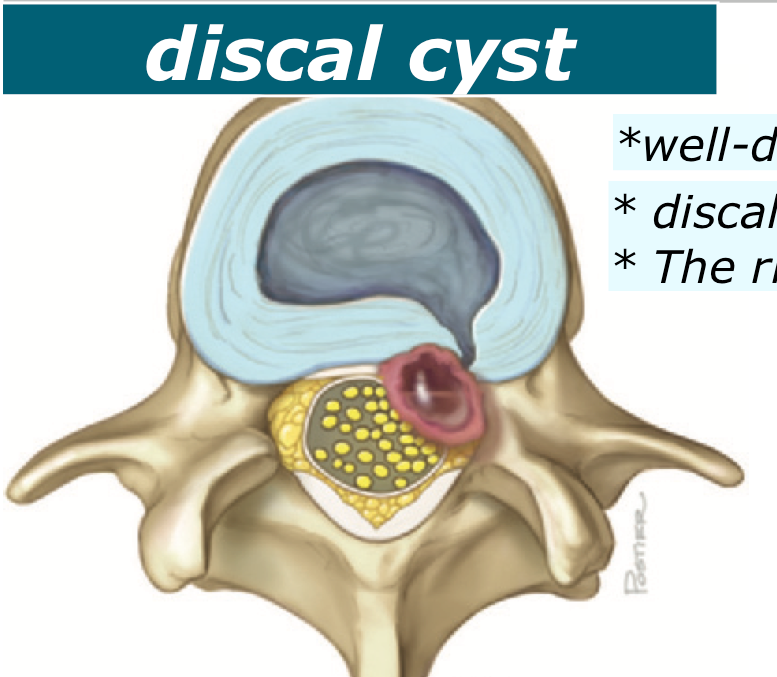
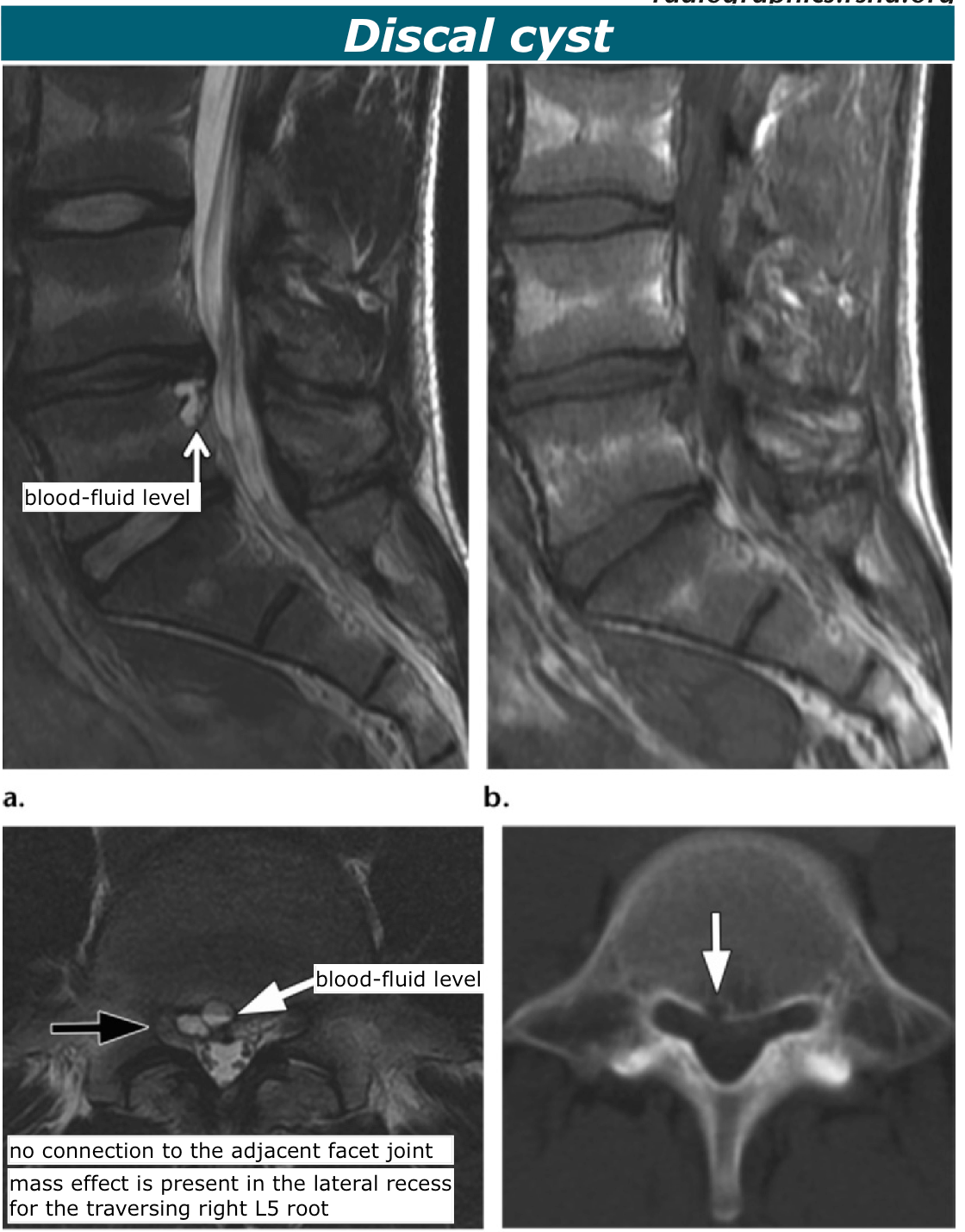
Discal Cyst >> well-defined intraspinal extradural cyst communicates with the intervertebral disk
discal cysts are thought to re- sult from an injury to the anulus fibrosus, with fluid accumulation and formation of a pseudo- membrane Discal cysts have a striking male predilection (~90%) and manifest in patients at a relatively young age, with a reported mean age of 33.5 years
Imaging Features/Discal cyst >>
A T2-hypointense rim is typically depicted a blood- fluid level, if present, can be a clue to the diagno- sis of a discal cyst Discal cysts are most common at L4- 5 Lack of connection to the facet joint should be sought Lack of appreciable degenerative disk disease can be a clue to the diagnosis
Discal cyst >>
Acute Intravertebral Disk Herniation: Acute Schmorl Node >>
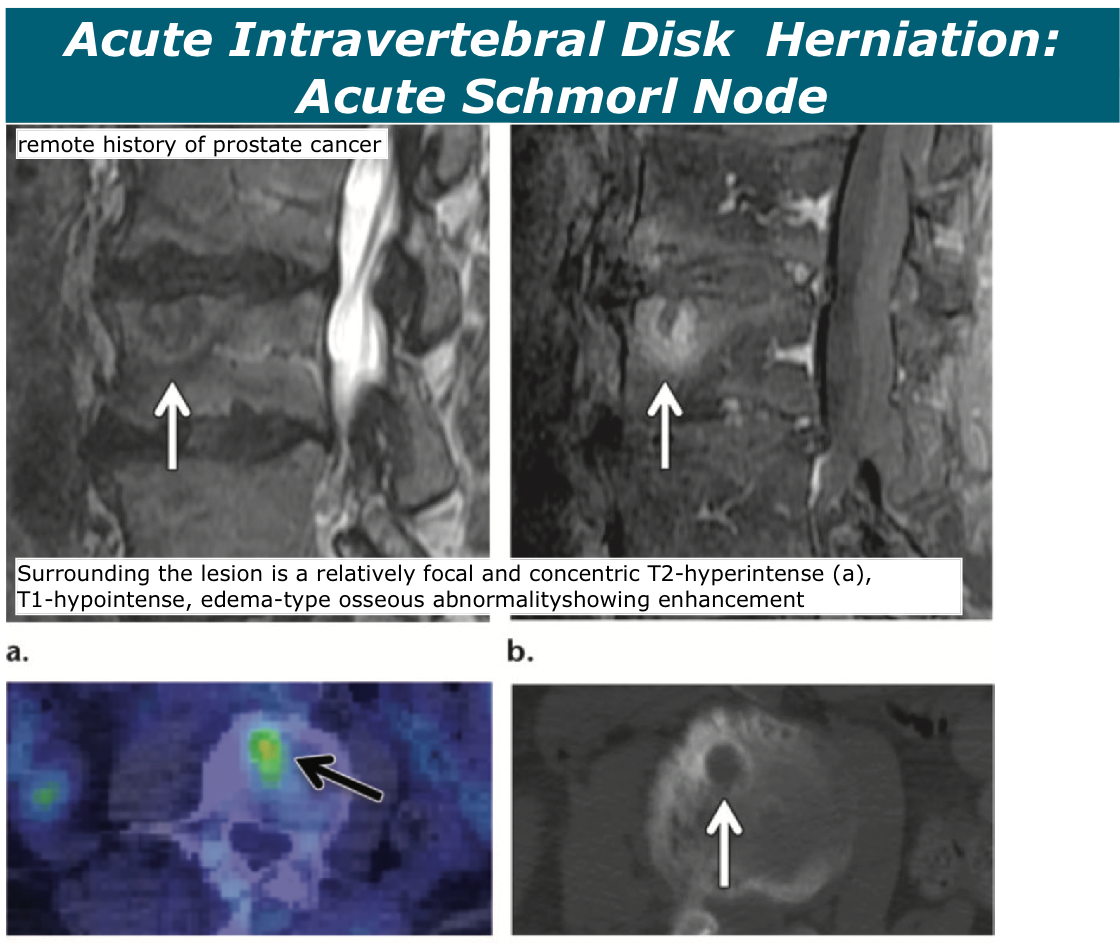
Imaging Features/Acute Schmorl node >> the disk initially may peripherally enhance in the acute phase (Fig 7) and then enhance more homogeneously for 6 months or more
The uptake that can be observed in acute Schmorl nodes on a bone scan and at PET (Fig 9) generally evolves to normal during a period of months
Differential Diagnosis/Acute Schmorl node >> Among edema-inciting Schmorl nodes, the formation of concentric rings of T2 hyperin- tensity surrounding the node at MR imaging has a moderately high negative predictive value for the absence of neoplasm, infection, and fracture (72% in one study)
paraspinal or epidural soft-tissue mass, paraspinal inflammatory changes, and evidence of osseous erosive changes (including at CT) can help favor a diagnosis of osteomyelitis over a recent Schmorl node.
Acute Schmorl node >>
Acute Schmorl Node >>
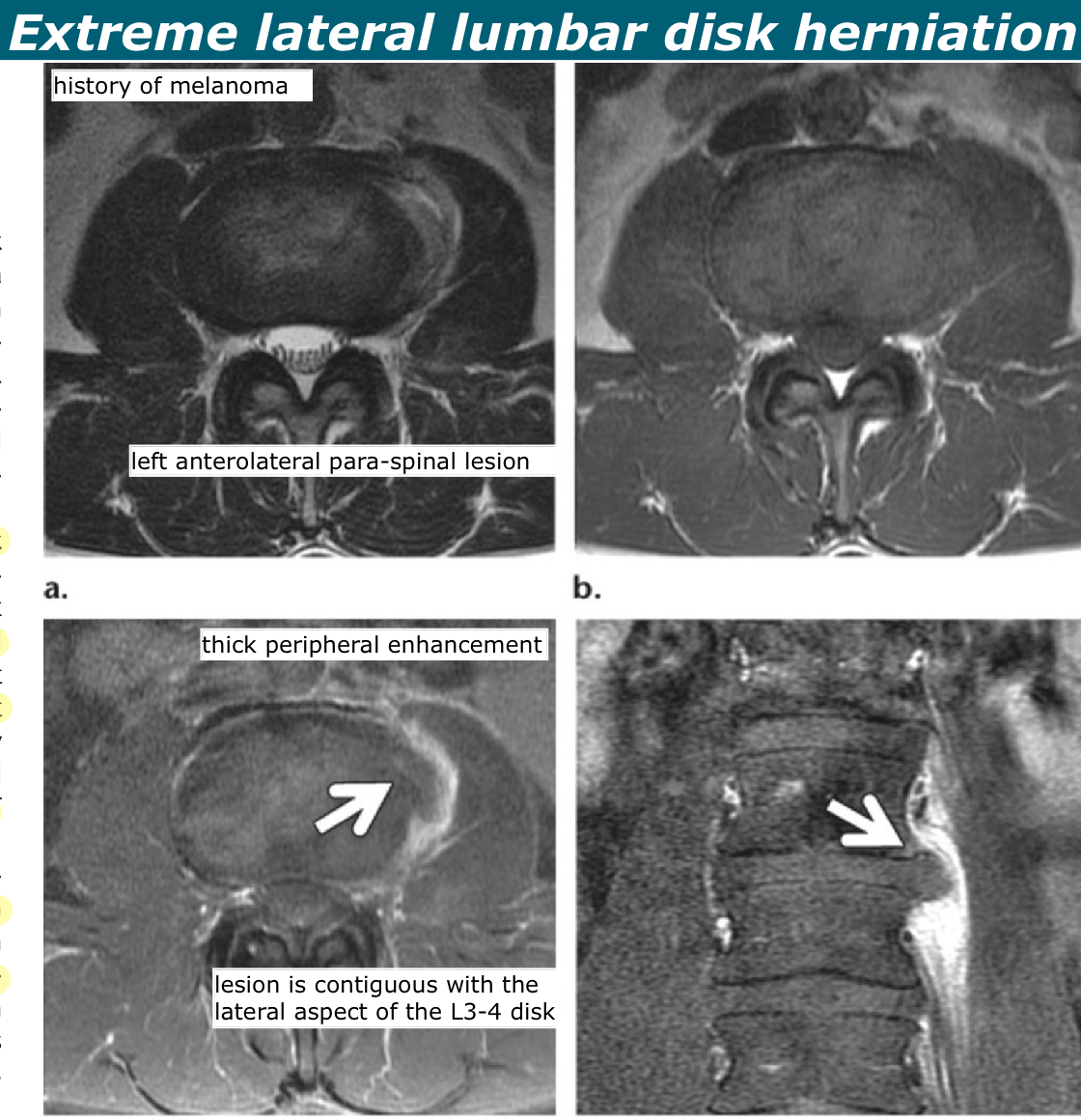
Extreme Lateral Lumbar Disk Herniation >>
Extreme Lateral Lumbar Disk Herniation >> terms such as extreme lateral, retroperitoneal, or anterior are used to refer to such herniations, especially when they occur at the anterior or anterolateral aspects of the spine
Differential Diagnosis/Extreme Lateral Lumbar Disk Herniation >> Extreme lateral herniated disks with a smoothly marginated, round morphologic structure may particularly simulate neoplasms.
A primary benign or malignant retroperitoneal neoplasm, metastasis, adenopathy, or a paraspinal or retroperitoneal abscess may also be consid- ered. prominent paraspinal venous plexus are additional mimics
Extreme Lateral Lumbar Disk Herniation >>
FDG-Avid Disk Herniation >>
FDG-Avid Disk Herniation >> disk herniations, particularly when acute or subacute and associ- ated with an inflammatory response, can cause focal uptake at PET
Such FDG avidity can simulate metastatic dis- ease or other more sinister pathologic conditions
Symptomatic Thoracic Disk Herniation >>
Symptomatic Thoracic Disk Herniation >> They are termed giant when the herniation oc- cupies more than 40% of the spinal canal at CT myelography or MR imaging
These giant thoracic disk herniations are often densely calcified (~95%) and tend to erode the dura Giant thoracic disk herniations can be associated with spontaneous intracranial hypotension For symptomatic tho- racic disk herniations, the most common manifesta- tion is pain, which is seen in approximately 75% of patients
Symptomatic Thoracic Disk Herniation >> Two-thirds of symptomatic thoracic disk herniations that require surgery are located between T8 and T11
The vast majority (~95%) has the bulk of the herniated material medial to the lateral margins of the thecal sac
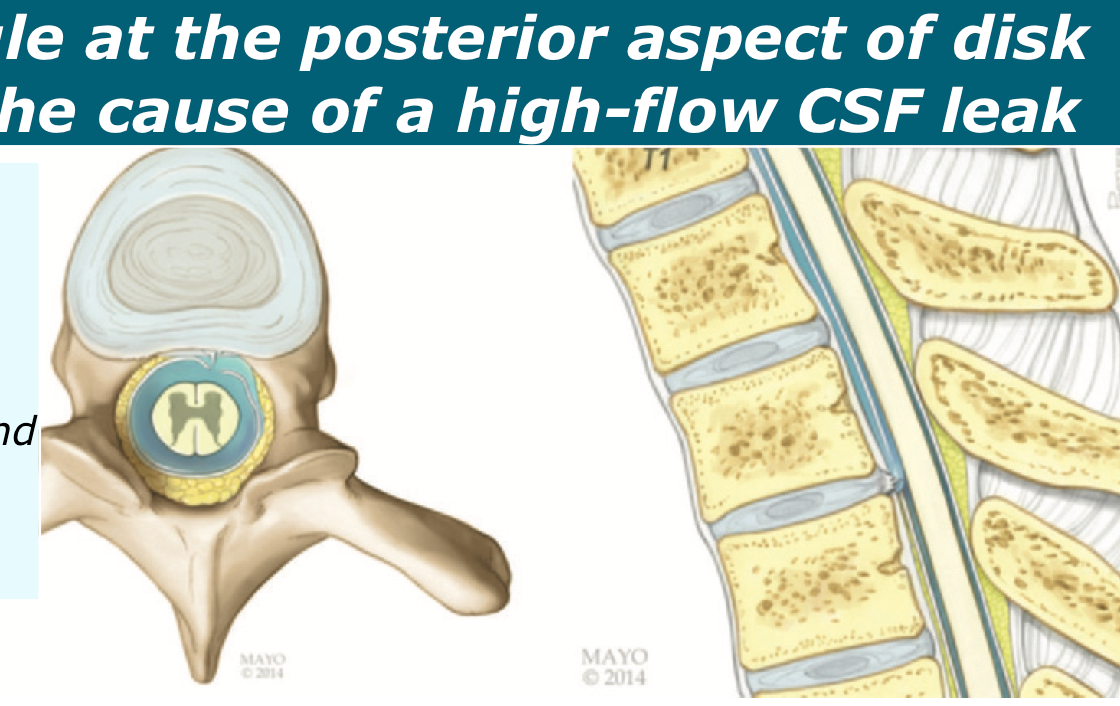
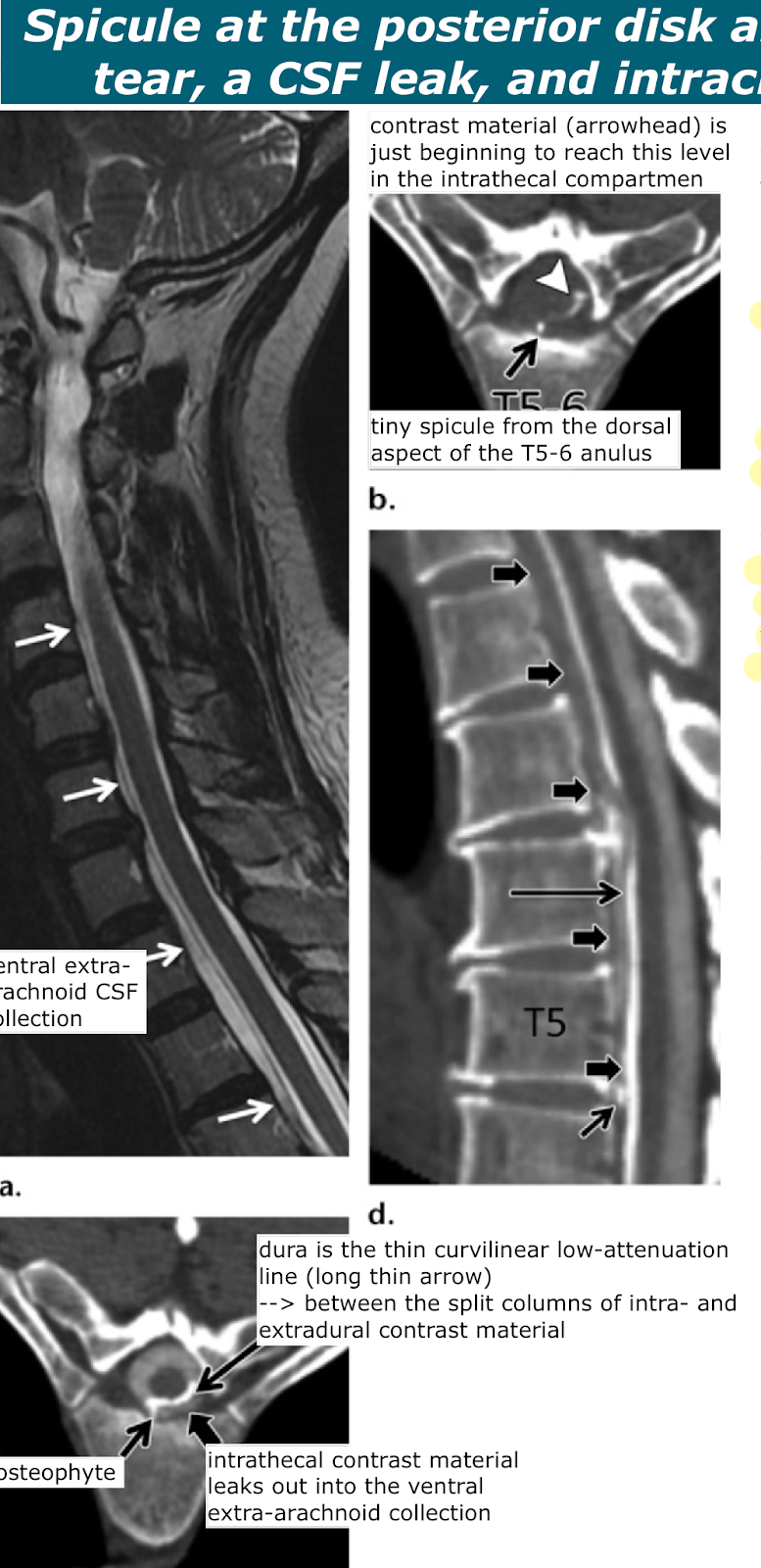
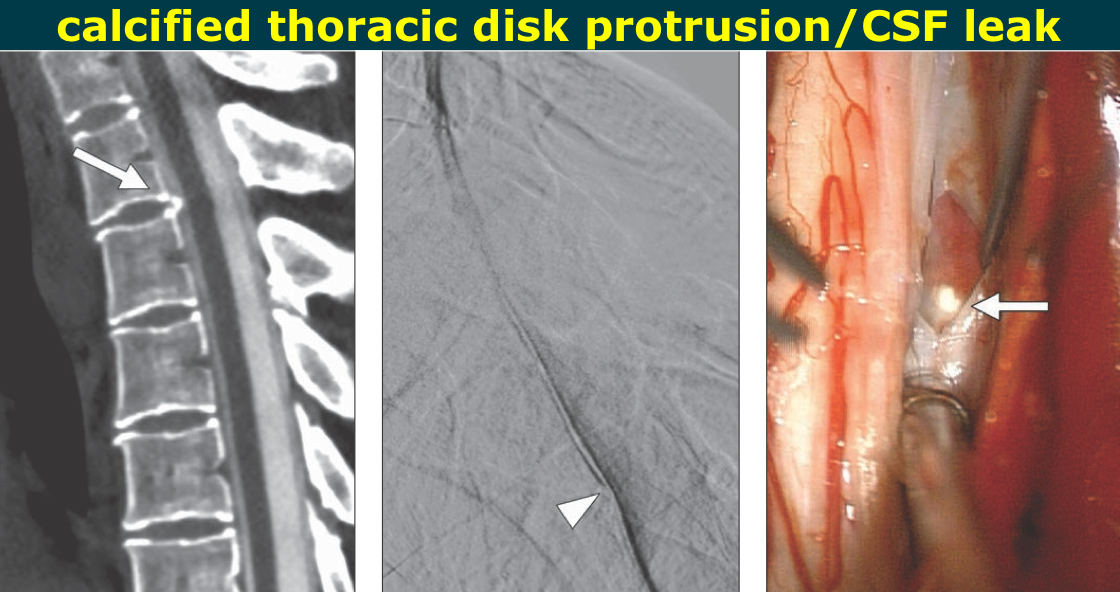
Spicule at the posterior disk anulus causing a dural tear, a CSF leak, and intracranial hypotension >> calcified disk remnant or osteophytic spur can cause a dural defect, the resultant CSF leak, and the clinical manifestations of CSF hypotension
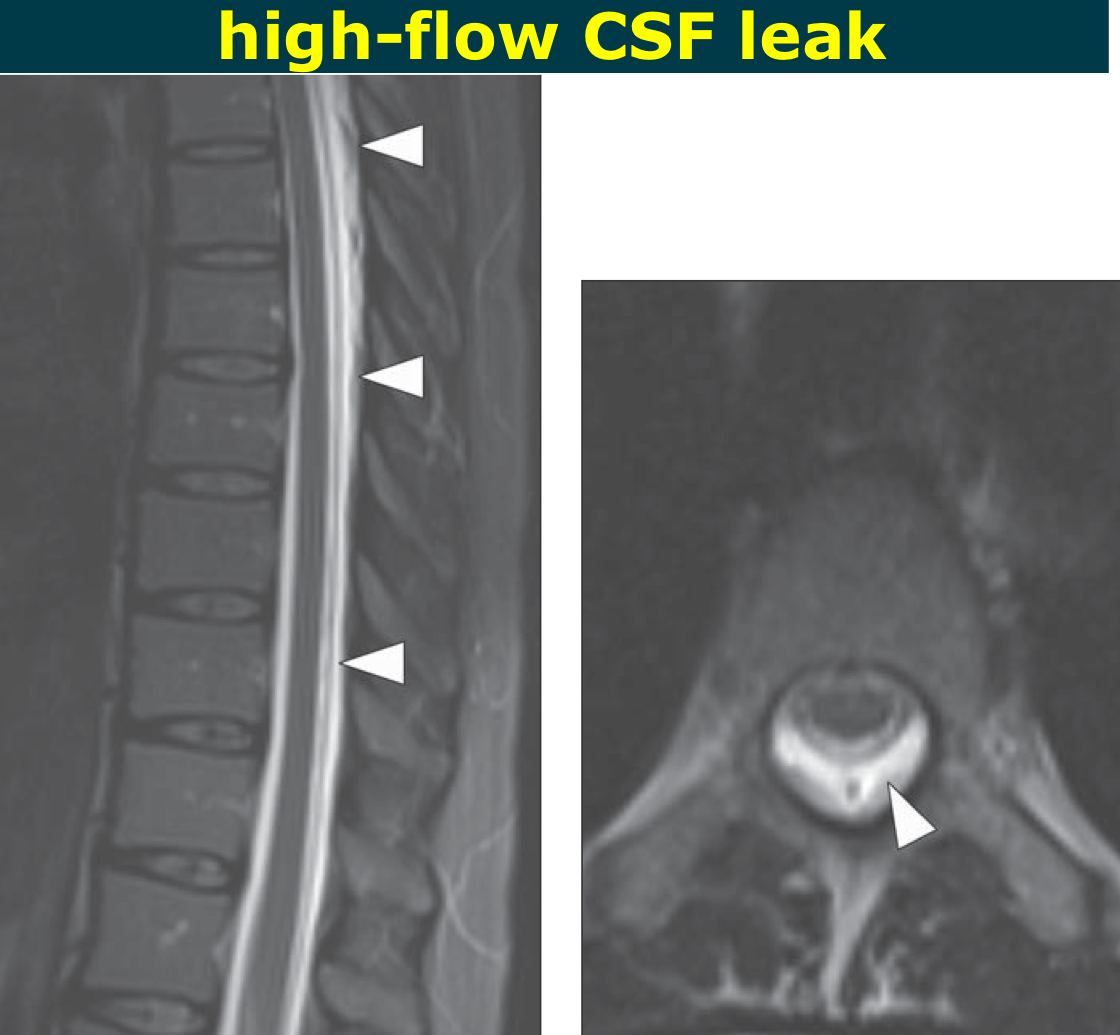
Such small dural defects can cause a spectrum of disease, including a CSF leak, intradural disk herniation (described earlier), and ventral spinal cord herniation nearly 90% of the high-flow CSF leaks were located between C5 and T7
Imaging Features/Spicule at the posterior disk anulus causing a dural tear, a CSF leak, and intracranial hypotension >> detection of the findings of CSF hypotension in the brain and spinal canal
extradural spinal CSF collec- tions The dural tear and the associated typically rapid CSF leak can be de- picted by using ultrafast dynamic CT myelogra- phy The spicules are typically tiny and sharp and are directed posteriorly double line sign may be observed, caused by the dura being interposed between the intra- and extradural contrast material
Spicule at the posterior disk anulus causing a dural tear, a CSF leak, and intracranial hypotension >>
>>
>>
Epidural fluid 참고이지미 >>
Dural sac is seen as thin black line separating intrathecal CSF from epidural collection. Thecal sac is partially collapsed because of loss of CSF.
Fluid Collections >> most frequently encountered finding
85% of the patients The collections tended to be nonfocal and often extended over five or more spinal segments. epidural location
extensive dorsal fluid collection >>
surgically documented leakage at T8.
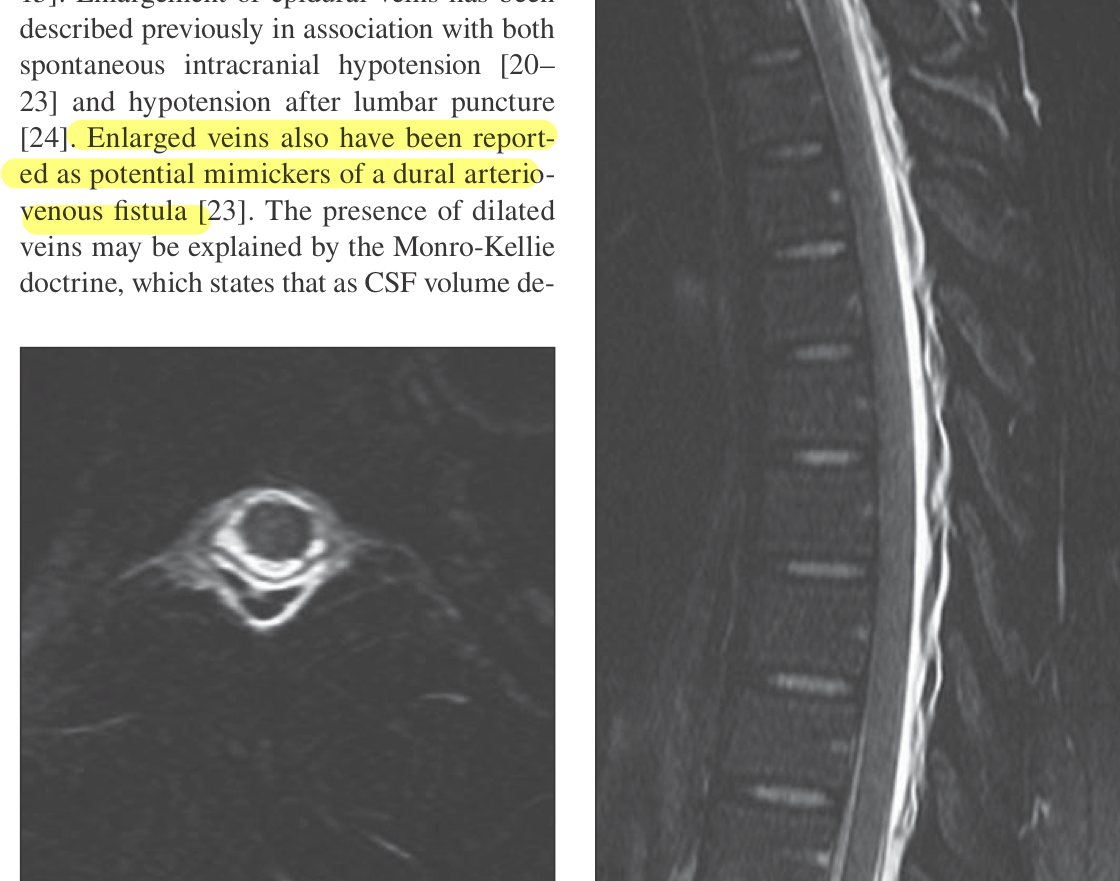
Dilated Epidural Veins >>
Dilated Epidural Veins >> 77% of the patients in this series
CSF volume decreases, blood volume increases in an attempt to maintain a stable pressure, essentially lead- ing to compensatory vasodilatation in the brain, spine, and meninges
Dilated Epidural Veins >>
prominent dorsal flow voids that represent dilated veins that appear to be extradural
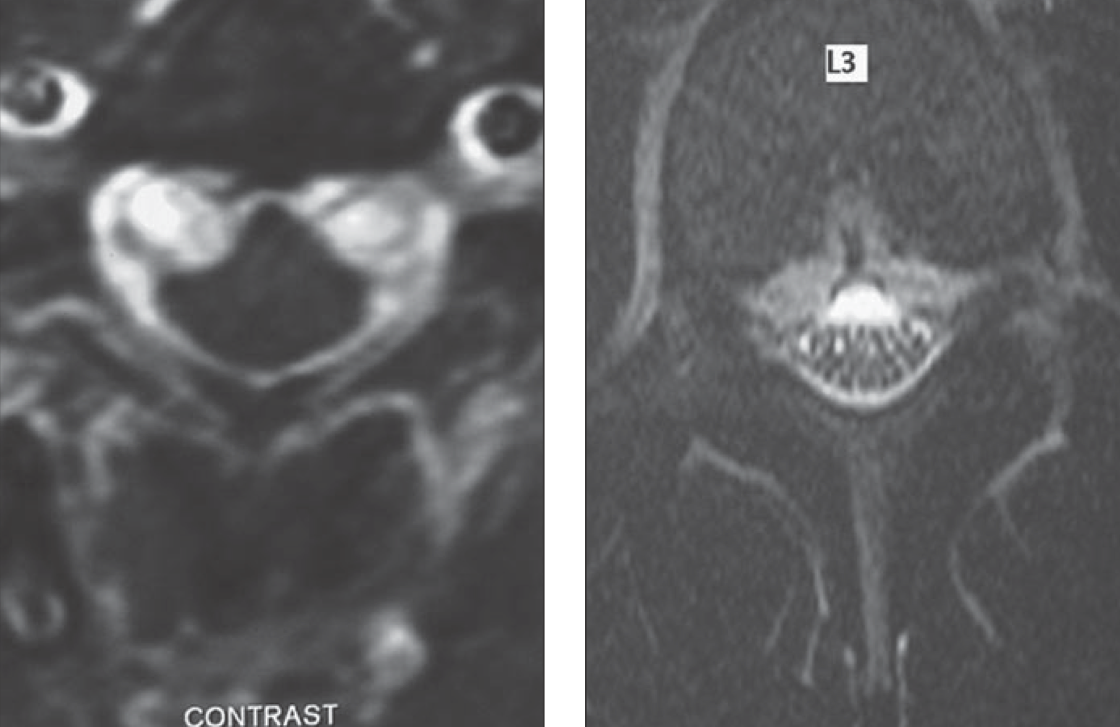
Epidural Venous Plexus >>
Epidural Venous Plexus >> The festooning results when the en- larged plexus causes collapse of the lateral aspects of the thecal sac while the sac main- tains its midline attachment to the posterior longitudinal ligament
Epidural Venous Plexus >>
festooned appearance of cervical epidural venous plexus at level of C3. Mass effect on thecal sac is evident
Dural Enhancement >>
Dural Enhancement >> dural enhancement is assumed to result from dural vasodilation and engorgement
The enhancement tended to be smooth and circumferential
Dural Enhancement >>
smooth dural enhancement that extends into neural foramina
Structural Abnormalities >>
Structural Abnormalities >> Association of Spontaneous intracranial hypotension with nerve root cysts, pseudo- meningocele, disk herniation, and transdural osteophytes has been reported
C1–C2 Sign >>
C1–C2 Sign >> also been called the C1–C2 false localizing sign [30, 31], is seen on MR images as a fo- cal area of fluidlike signal intensity and on CT myelograms as a CSF collection between the spinous processes of C1 and C2
It should be not- ed that this fluid collection does not neces- sarily denote the site of CSF leakage The C1–C2 level may be prone to the escape of fluid because of lack of osseous support, mobility of the segment, lack of epidural fat, and laxity of the connective tissues at this level
C1–C2 Sign >>
fluid signal intensity collection between spinous processes of C1 and C2
Lack of Intracranial Findings >>
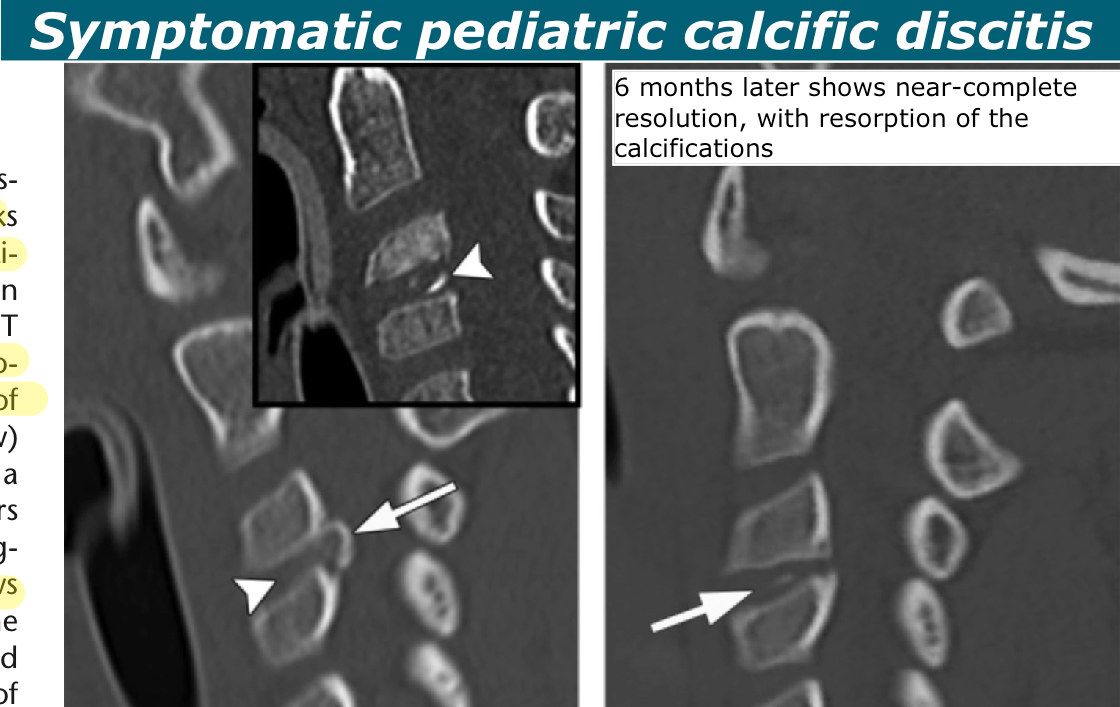
Pediatric Acute Calcific Discitis >>
Pediatric Acute Calcific Discitis >> The mean age of pedi- atric patients is 7 years (70), and there is a male predominance
favorable prognosis, and diagnostic or therapeutic intervention is to be avoided self-limiting inflammatory disease Symptom onset was typically abrupt, from a few hours to 2 days in many cases Evidence of inflammation in the form of fever, an elevated white blood cell count, or elevated levels of inflammatory markers may be found.
Pediatric Acute Calcific Discitis >> Pediatric calcific discitis typically involves exclusively or primarily the nucleus pulposus, rather than the anulus, as is the case for asymptomatic incidental disk calcification
The symptomatic form occurs primarily in the cervical spine (70%)
Imaging Features/Pediatric Acute Calcific Discitis >> disk space calcification, with or without disk space expansion,
relatively dense and relatively oval Marrow signal intensity changes in the adjacent vertebral bodies may also be depicted in some cases are edema- type changes or enhancing
Symptomatic pediatric calcific discitis >>
>>
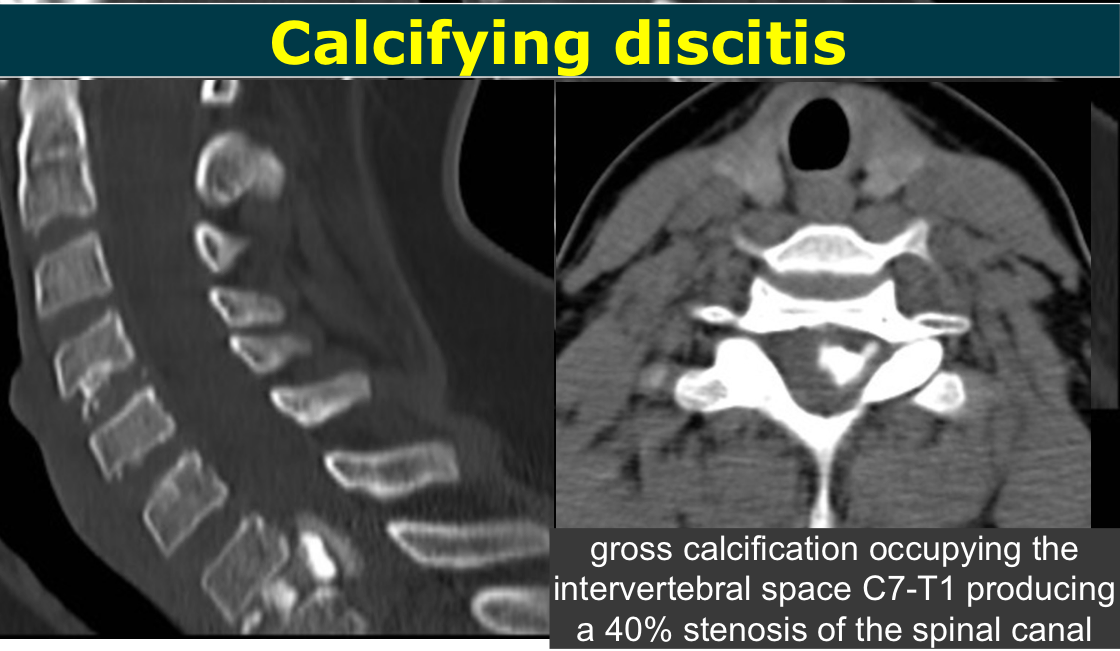
Calcifying discitis >>
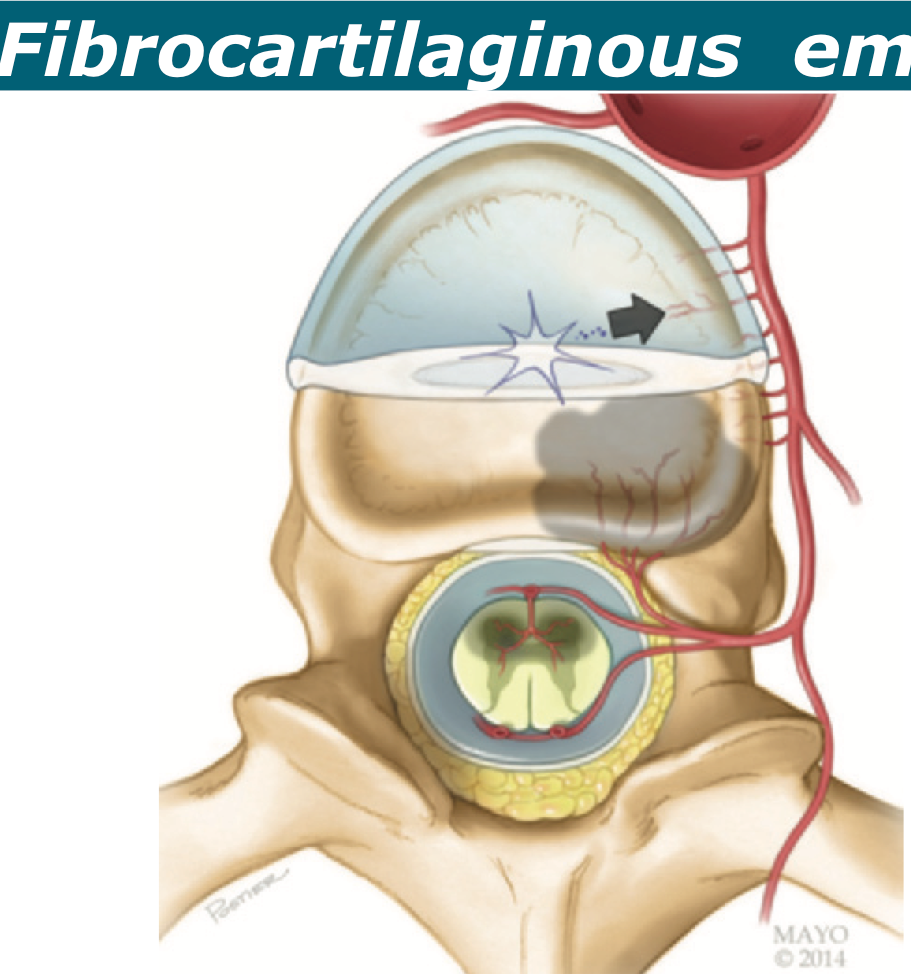
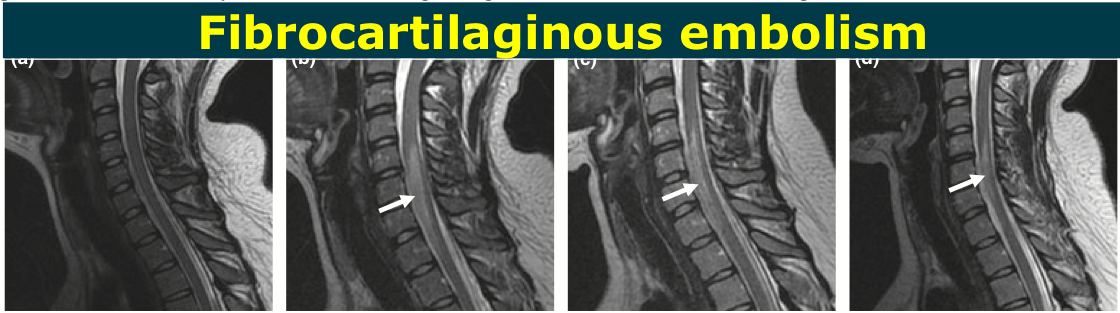
Fibrocartilaginous Emboli of Disk Material to the Spinal Cord >>
Fibrocartilaginous embolism of disk material to the spinal cord >>
fibrocartilaginous embolism >> Fibrocartilaginous embolism of disk material to the spinal cord is also known as a nucleus pulposus embolism
fibrocartilaginous embolism of disk material to the spinal cord is considered a frequent condition in veterinary medicine, particularly in dogs It is possible that a considerable number of “idiopathic” spinal cord infarcts or even cases of acute “transverse myelitis” are due to fibrocartilaginous emboli
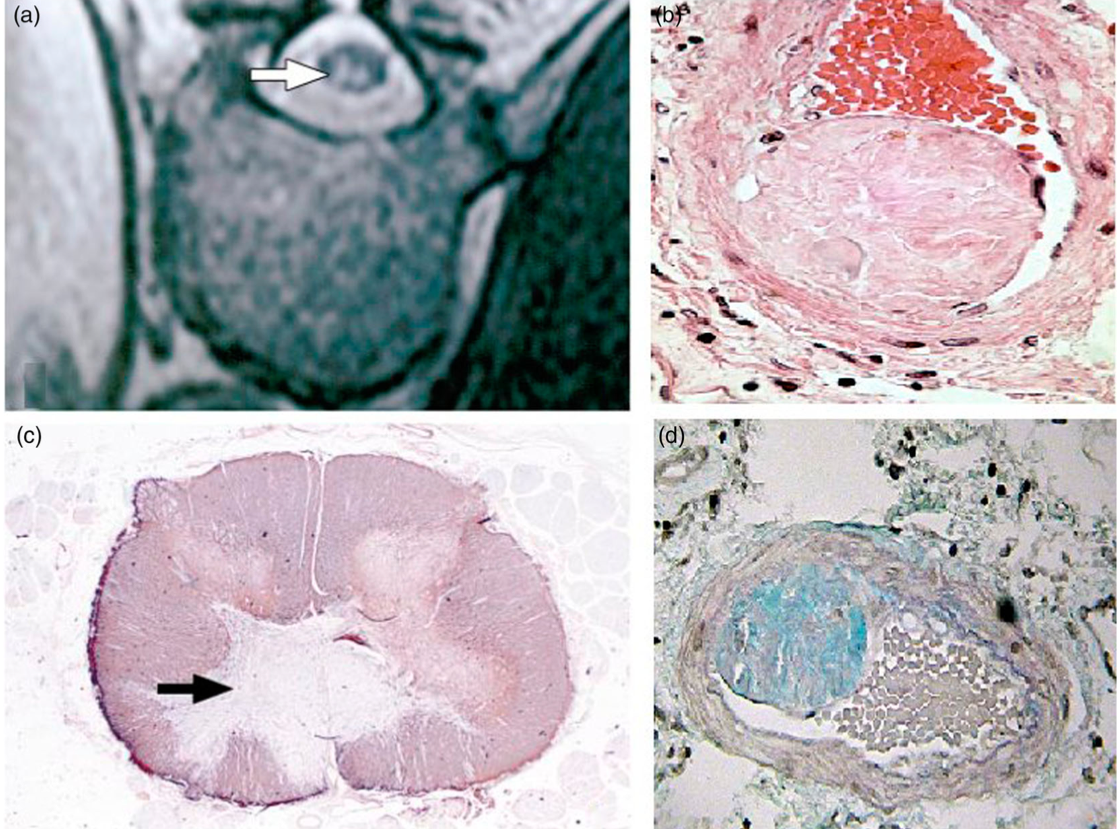
fibrocartilaginous embolism >> In a possible etiology, an embolus of disk material enters a segmental artery retrograde (arrow), either by way of direct arterial flow or from sinusoids into arteriovenous shunts.
The embolus then reaches the spinal cord through antegrade flow, resulting in an infarct of the spinal cord at multiple levels, usually in the anterior spinal artery distribution The embolic material can also extend into the vertebral body blood supply, causing a bone marrow infarct
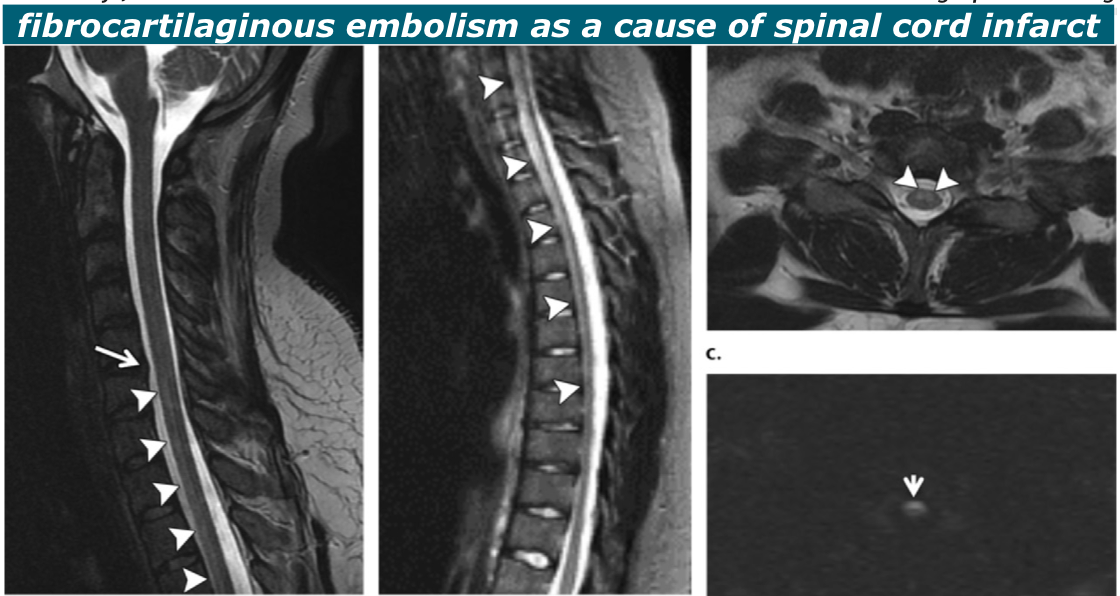
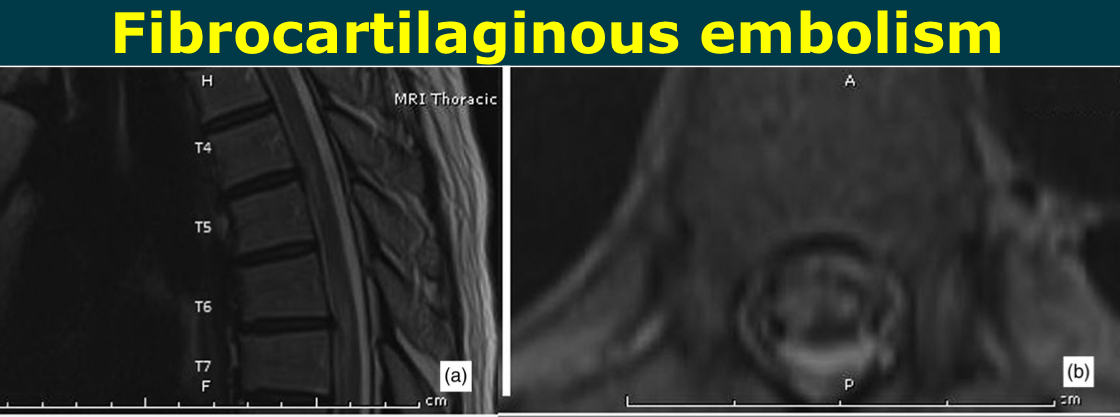
fibrocartilaginous embolism >> The cervical spinal cord is involved in approximately 70%
On average, the infarct affects a span of five to six vertebral segments. The anterior spinal artery ter- ritory is most commonly involved
Imaging Features/fibrocartilaginous embolism >> MR diffusion - restriction in the acute and early subacute phase
infarct progresses into the later acute and subacute phases with spinal cord expansion, T2 hyperintensity (Fig 14a–c), and contrast enhancement Vertebral body infarcts may be seen If hemorrhage is present, complex signal intensity characteristics, in- cluding T1 hyperintensity, may be seen.
—> it has been suggested that a venous infarct, rather than an arterial infarct
fibrocartilaginous embolism >> diagnosis of exclusion.
—>Thus, other causes of spinal cord infarct should be sought at imaging and clinically, including aortic or vertebral dissection, recent aortic surgery, cardiac valve disease, atrial fibrilla- tion, hypotension, infectious or rheumatologic or autoimmune causes, or inherited hypercoagulable states
nonvascular my- elopathy such as that caused by a demyelinating disease or an inflammatory or infectious process, a neoplasm, and vascular malformations.