#AnkleMRI, #Mueller-Weiss, #Hindfootvarus, #Navicular, #footpain, #footosteoarthritis, #chroicfootpain
#안산에이스병원,#Ansan_Ace_Hospital, #MSK_MRI, #mskmri_Ankle, #영상의학과이지은, #영상의학공부맛집,







Mueller Weiss syndrome is a spontaneous adult onset osteonecrosis of the tarsal navicular.
This syndrome is multifactorial and related to chronic loading on a suboptimally ossified navicular bone susceptible to central osteonecrosis due to its centripetal blood supply. It is distinct from Köhler disease, the osteochondrosis of the tarsal navicular bone that occurs in children.
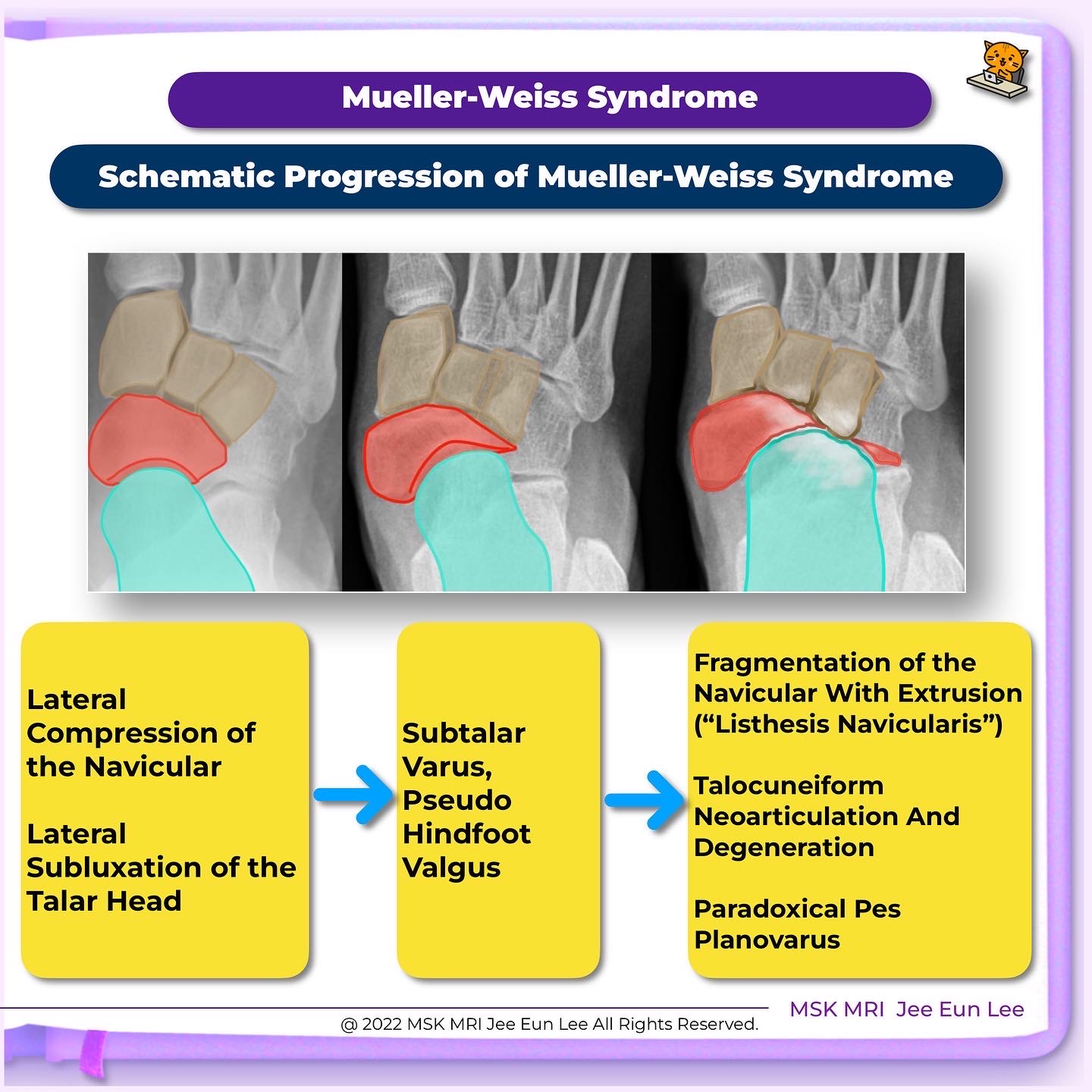
Mid- and hindfoot show gradual collapse and, ultimately, fragmentation of the lateral aspect of the navicular
With progressive compression and fragmentation of the navicular, there is lateral subluxation of the talar head that results in subtalar varus, pseudohindfoot valgus, and talocuneiform neoarticulation.
The first metatarsal is usually primarily short (index minus) or secondarily short with respect to the second metatarsal due to the internal rotation of the medial part of the navicular bone.
As the lateral half of the navicular collapses, it becomes sclerotic and comma- or hourglass-shaped in appearance with an internal rotation of the medial half of the bone.
A Cyma line is an S-shaped line composed of well-aligned talonavicular and calcaneocuboid joints.
Disruption of cyma line
The navicular contributes to the integrity of both the transverse and medial longitudinal arches of the foot.
Anteriorly, the navicular has a convex nephroid appearance with two crests creating three articular surfaces for cuneiform bones(medial, middle, and lateral), each articulating with a corresponding cuneiform bone.
In MWS, beginnings of neoarticulation between laterally subluxed talar head and lateral cuneiform, and degenerative changes at talonavicular joint and early talocuneiform neoarticulation.
MRI allows for the identification of edema in the initial phases of MWD, the presence of chondral defects, and the involvement of the Lisfranc and the calcaneocuboid joints.
CT scan allows for a more adequate visualization of joint surfaces and the morphology of the navicular bone as well as the talonavicular and naviculocuneiform joints.
We can assess the size of the lateral half of the navicular, its fragmentation, osteophytes, subchondral changes.
prominent navicular tuberosity may give the false clinical impression of hindfoot valgus, or pseudohindfoot valgus, but the head of the talus is displaced laterally and placed over the hindfoot midaxis pointing laterally
This is best appreciated on a weight-bearing DP foot radiograph
Normal AP talo-calcaneal angle (Kite’s angle) is 15-30 degrees.
An angle greater than 30 degrees indicates hindfoot valgus and lesser than 15 degrees indicates hindfoot varus.
The medial longitudinal arch can be markedly flattened depending on the severity of the disease.
This combination of pseudohindfoot valgus and pes planus deformity is also known as paradoxical pes planovarus.